ACL injuries in football

ACL Injuries in Football: What You Need to Know — and How to Get Back on the Pitch
An ACL injury is one of the most feared diagnoses in football. The crack, the instant instability, the sinking feeling — and then the long road ahead. But here’s what we know: with the right rehab, most players return to the game they love. This article covers everything you need to understand about ACL injuries — what causes them, what recovery looks like, and what it takes to get back on the pitch safely.
What Is the ACL — and Why Does It Matter?
The anterior cruciate ligament (ACL) is a band of connective tissue that connects your tibia (shin bone) to your femur (thigh bone) inside the knee. It does two critical jobs.
Mechanical stability: it stops your tibia from sliding forward on your femur and controls rotational forces through the knee.
Sensory signalling: the ACL is densely packed with nerve receptors that act as a data centre for your brain, relaying real-time information about your knee’s position, tension, and movement as you run, jump, twist, and change direction.
When the ACL is damaged, you lose both. The knee feels unstable. Your brain loses the fine-grained feedback it relies on to coordinate movement. That’s why ACL rehab isn’t just about rebuilding strength — it’s about retraining the whole neuromuscular system.
How Do ACL Injuries Happen in Football?
Not how you might think. A landmark 2020 study published in the British Journal of Sports Medicine examined 134 ACL injuries in elite football players and found:
- 44% were non-contact injuries
- 44% were indirect contact injuries
- Only 12% involved direct contact to the knee
That’s 88% of injuries with no direct blow to the knee. So what’s actually causing them?
The mechanics of injury
The most common triggers were:
- Pressing (47%): the high-intensity movement to win the ball from an opponent
- Being tackled (20%): defensive body contact while in possession
- Kicking and balance (16%): maintaining stability during or after a strike
- Landing from a jump (7%): particularly on one leg with rotational forces
A key finding was mechanical perturbation — when a player’s upper body is bumped or pulled while their lower body is planted on the ground, the resulting twisting force through the knee dramatically increases ACL injury risk. Pressing, tackling, and defensive actions are all high-risk moments, not because players are colliding knee-to-knee, but because of the aggressive whole-body movement interactions involved.
The high-risk position: dynamic knee valgus
The most common mechanism of injury is dynamic knee valgus — where the knee collapses inward as the hip rotates internally and the foot is planted. This position places enormous stress on the ACL. It’s most likely to occur during deceleration, landing, or a rapid change of direction. It can also happen subtly during pressing and tackling when the player is off-balance.
Identifying and correcting this movement pattern is a cornerstone of both ACL rehab and injury prevention.
Timing: when in the match do injuries happen?
The same 2020 BJSM study found that 25% of all ACL injuries occurred in the first 15 minutes of the match — before fatigue can be blamed. This matters because it shifts the conversation away from ‘the player was tired’ and towards readiness: how prepared is the neuromuscular system at kick-off?
Proper warm-up, cognitive readiness, and pre-match activation are not optional extras. They are injury prevention.
A Note on Female Athletes

Example of dynamic valgus load on knee.
Female footballers face a significantly higher risk of ACL injury than their male counterparts — estimates range from two to eight times higher, depending on the sport and study. Contributing factors include differences in hormonal fluctuation across the menstrual cycle, biomechanical differences in landing patterns, and neuromuscular control. At Vitality Physiotherapy, our team has specific expertise in female athlete ACL rehab and prevention — something we factor into every programme we design.
Is an ACL Tear Career-Ending?
“Be patient, don’t cut corners, and do everything the Physio tells you.” — Alan Shearer CBE
No. And there’s compelling evidence to back that up.
A widely cited study reported that 83% of athletes return to professional sport following ACL reconstruction. The key variable isn’t the injury itself — it’s the quality of the rehabilitation.
Consider Alan Shearer. On Boxing Day 1992, playing for Blackburn Rovers against Leeds United, he ruptured his ACL in the first half — and didn’t realise it. He went on to score twice in a 3-1 win. After surgery and a structured rehab programme, he returned the following season to score 31 goals in 40 games. He credits that return to one principle: do the work, follow your physio, don’t rush it.
The players who struggle to return are, more often than not, those who return too soon — before their knee is truly ready.
How Long Does ACL Rehab Take?
The standard timeframe is 9 months — but this is a minimum, not a target. Virgil van Dijk returned at 9 months after his 2020 injury. Others take 12–18 months to reach full competitive fitness. The timeline depends on:
- Whether you had surgery or are managing conservatively
- The extent of any associated injuries (meniscus, other ligaments)
- Your pre-injury fitness level
- How consistently and intelligently you complete your rehab
- Your neuromuscular readiness — not just structural healing
The research is clear: returning at 9 months carries a significantly lower re-injury risk than returning at 6 months. Every week of quality rehab reduces that risk. There is no shortcut that doesn’t cost you later.
What Does ‘Ready to Return’ Actually Mean?
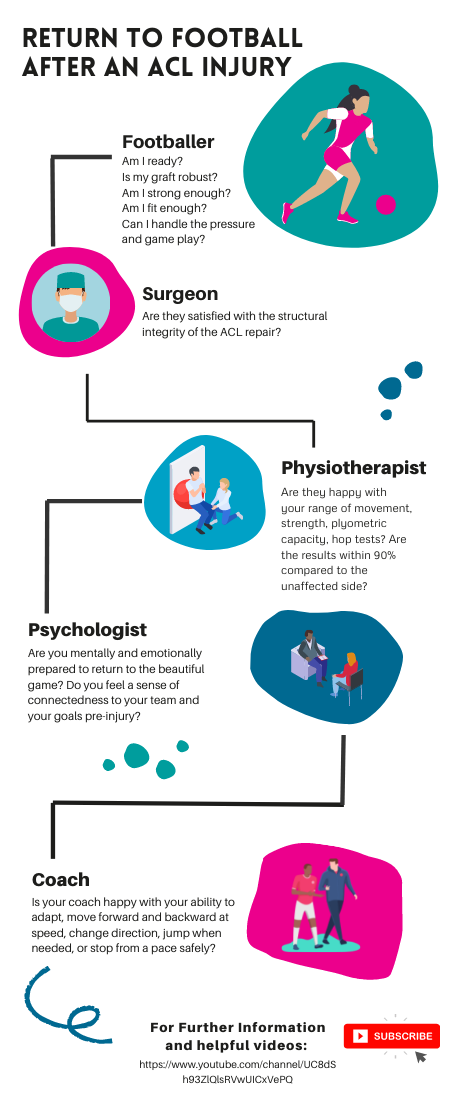
Return to football infographic by Vitality Physiotherapy
Return-to-play is not a date on a calendar. It’s a decision made by a team — athlete, physiotherapist, surgeon, coach, and sometimes a sports psychologist — using objective data. Here’s what that looks like in practice.
The athlete
Do you trust your knee? Can you commit to a tackle, a sprint, a jump — without hesitation or fear? Psychological readiness is not a nice-to-have. Fear of re-injury is one of the strongest predictors of not returning to pre-injury performance levels. Your inner voice matters as much as your single-leg hop score.
The physiotherapist
Your physio needs to see objective evidence of readiness across multiple domains:
- Strength and power: can you achieve 90%+ limb symmetry on strength testing?
- Hop testing battery: single leg vertical hop, forward hop, timed 6m hop, triple hop, triple crossover hop, lateral hop, medial hop, and their rotational variants. This isn’t an arbitrary list — each test assesses a different demand of football movement.
- Neuromuscular control: reaction times, adaptability under fatigue, dynamic balance
- Movement quality: can you decelerate, change direction, and land without compensating?
The surgeon
Structural integrity matters. Your surgeon will assess graft healing, range of movement, and whether the reconstructed ACL has the mechanical properties required for full sport. A happy surgeon means a structurally sound knee — but structural soundness alone is not clearance to play.
The coach
Pitch-based performance has to match the test results. Can you accelerate and decelerate at full speed? Change direction under pressure? Jump and land when required? React to a ball coming at you unpredictably? Return to training is the bridge between rehab and competition — it shouldn’t be skipped.
The role of cognitive training
A 2021 study found that cognitive skills, reaction time, and processing speed are significant factors in preventing ACL re-injury. This is why progressive, evidence-based ACL rehab includes reactive drills — small-sided games, decision-making under pressure, gates games, possession exercises. The nervous system needs to be retrained, not just the muscles.
Physical fitness without cognitive and neuromuscular readiness is a re-injury waiting to happen.
The Final Whistle
An ACL tear is not relegation. It is a significant injury — but it is one that, with the right support and the right approach, most players recover from fully.
The players who come back stronger are the ones who take the rehab seriously, trust the process, and resist the temptation to rush. There are no shortcuts — but there is a clear path.
At Vitality Physiotherapy, we have the clinical experience, the protocols, and the team to take you from injury to full return to football — whether you’re playing Sunday league or semi-professionally. We work across our Southwark (SE1) and Esher (KT10) clinics, and we’d love to support your recovery.
Want to talk through your injury? Book a free 15-minute call with one of our ACL specialists — from the convenience of home.
Call us: 020 7193 9928
Email: info@vitality-physio.co.uk
References
Della Villa F et al. (2020). Football ACL injuries reloaded. British Journal of Sports Medicine Blog.
Ardern CL et al. (2018). Return to sport following ACL reconstruction. British Journal of Sports Medicine.
Grooms D et al. (2021). Cognitive and neurological contributors to ACL re-injury. Journal of Orthopaedic & Sports Physical Therapy.