
Tennis Elbow (Lateral Elbow Tendinopathy)
Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy
Pain on the outer elbow that catches when you grip, lift, or twist is one of the most common presentations we see in clinic. It interrupts ordinary tasks — carrying shopping, opening jars, using a mouse — in a way that quickly becomes difficult to ignore.
Tennis elbow tends to build gradually, often over weeks, before it becomes persistent enough to seek help. With the right assessment and a structured approach to rehabilitation, the vast majority of cases resolve well.
What is tennis elbow?
 Tennis elbow — clinically known as lateral elbow tendinopathy — is a condition affecting the tendons that attach the forearm extensor muscles to the outer elbow. The tendon most commonly involved is the extensor carpi radialis brevis (ECRB), which plays a central role in controlling wrist and hand movement.
Tennis elbow — clinically known as lateral elbow tendinopathy — is a condition affecting the tendons that attach the forearm extensor muscles to the outer elbow. The tendon most commonly involved is the extensor carpi radialis brevis (ECRB), which plays a central role in controlling wrist and hand movement.
Despite the name, most people who develop it have never played tennis. It affects office workers, tradespeople, gardeners, and gym-goers equally — anyone who places repeated demand on the forearm extensors beyond what the tendon is currently conditioned to handle.
Tennis elbow is fundamentally a condition of load and adaptation. The tendon is being stressed faster than it can recover — and that mismatch is what drives the pain.
It is not simply an inflammatory condition, which is why anti-inflammatory treatments in isolation rarely resolve it. Understanding this distinction is important — it shapes the entire approach to rehabilitation.
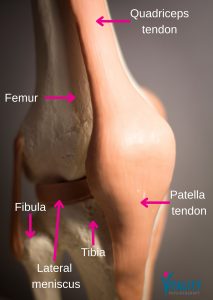
The anatomy
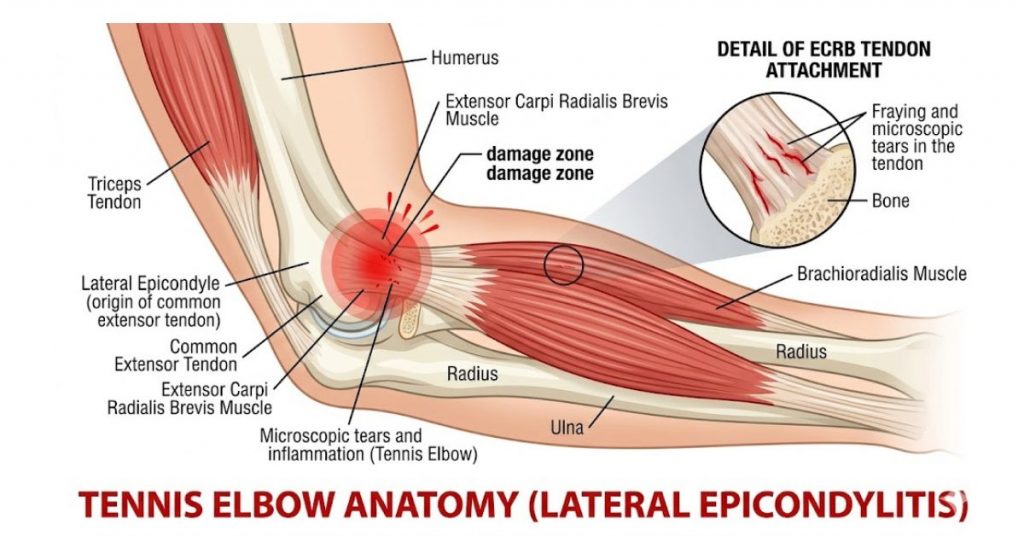
The muscles along the back of the forearm are responsible for extending the wrist and fingers and generating grip force. They attach collectively to a bony prominence on the outer elbow called the lateral epicondyle.
When these tendons are exposed to load they cannot currently tolerate, they undergo structural change at a tissue level. This leads to pain, stiffness, and a progressive reduction in the ability to perform activities that were previously unremarkable.
Symptoms
Tennis elbow typically develops gradually. The most common presentation includes pain on the outer aspect of the elbow, particularly with gripping or lifting; tenderness directly over the lateral epicondyle; weakness when carrying, opening jars, or using a mouse for extended periods; and morning stiffness that often eases with movement. In more established cases, localised swelling or a palpable thickening in the tendon may be present.
Symptoms often fluctuate in the early stages, which makes it tempting to push through on better days. This typically delays recovery.
Do I have tennis elbow?
The Chair Lift
For this test, you need a chair. The use of one that is not too heavy.
Start off by straightening your arm and bending your wrist (your fingers should be pointing downwards.) Lift the chair with your middle, index finger, and thumb. Try not to use your pinky and ring finger in this one. If there is any sharp pain or you are not able to lift the chair at all, then you may have Lateral Epicondylitis.
Why does it develop?
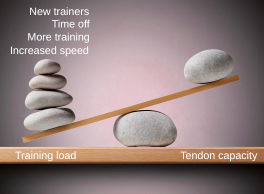
Tennis elbow develops when the cumulative demand placed on the tendon exceeds its current load capacity. This can result from a sudden increase in activity — a new role involving repetitive manual tasks, a return to racquet sport, or a change in training volume — or from sustained lower-level loading without adequate recovery time.
Common contributing activities include repetitive gripping, lifting and carrying, prolonged keyboard or mouse use, screwdriver work, gardening, and decorating. It is most frequently seen in adults aged 35 to 60, though it can affect anyone whose forearm extensors are regularly being asked to perform beyond their current conditioning.
Assessment
Diagnosis is made through clinical assessment. Imaging is rarely required and adds little to what a thorough hands-on examination can determine.
Your physiotherapist will take a detailed history — covering the onset and behaviour of symptoms, aggravating activities, and your work and sporting demands. Clinical tests typically include palpation of the lateral epicondyle, grip strength measurement, and resisted wrist and middle finger extension testing.
Assessment also looks beyond the elbow itself. Shoulder strength, cervical spine function, wrist mobility, and overall movement patterns all influence how much load is transferred through the lateral elbow. Identifying and addressing these contributing factors is often the critical step in achieving full, lasting recovery.
Treatment
The goal of physiotherapy is not only to settle the pain but to restore the tendon’s capacity to tolerate the demands being placed on it.
Load management
The first step is identifying activities that are currently aggravating the tendon and modifying them strategically. This is not the same as rest. Tendons respond poorly to complete unloading — the aim is to maintain activity at a level the tendon can tolerate while recovery progresses.
Pain management
Isometric exercises — generating force without joint movement — are effective at reducing tendon pain in the early stages and can be used to maintain muscle function while load is being managed. A supportive brace or taping technique may reduce strain during aggravating activities, and heat therapy can ease discomfort following loading.
Manual therapy
Hands-on treatment, including joint mobilisation, soft tissue work, and movement retraining, can improve mobility and reduce pain — particularly in the earlier stages of rehabilitation. It is most effective as a complement to a structured exercise programme rather than as a standalone intervention.
Progressive strengthening
This is where lasting recovery is built. Tendons adapt to progressive mechanical load — that stimulus drives the structural remodelling that restores capacity and resilience. Rehabilitation moves from isometric and eccentric exercises through to heavy slow-resistance training, before progressing to movements that reflect the specific demands of your work, sport, or daily life.
Tendons recover through load — the right kind, at the right pace. Progressive strengthening is not one option among many; it is the mechanism by which the tendon actually rebuilds.
Our Rehabilitation Facility
Vitality Physiotherapy’s clinics include a private rehabilitation gym equipped for clinical use and reserved exclusively for patient rehabilitation — not shared with the public.
This allows your physiotherapist to guide and progress your loading programme within the same clinical environment across all stages of recovery: from early pain management through to grip and wrist strengthening, upper limb conditioning, and sport-specific or work-specific return-to-activity testing.
For patients returning to manual work, racquet sport, or high-demand training, supervised gym-based rehabilitation provides a level of structured progression and oversight that home exercise programmes cannot replicate — and significantly reduces the risk of recurrence without the limitations of home exercise or the distractions of a commercial setting.
Common rehabilitation errors
Many cases of tennis elbow become persistent as a result of avoidable mistakes in management.
Complete rest reduces tendon capacity over time and typically makes the return to activity more difficult, not less. Returning to full load before the tendon has rebuilt sufficient capacity leads to symptom recurrence. Passive treatments — massage, ice, bracing — can reduce pain temporarily, but without a progressive strengthening programme the underlying deficit remains. Inconsistent exercise is one of the most frequent reasons tendon rehabilitation fails to progress; these tissues require regular, structured loading to adapt.
When to seek assessment
A physiotherapy assessment is advisable if elbow pain has persisted for more than a few weeks, if symptoms are affecting work or exercise capacity, if grip strength is measurably reducing, or if self-management has not produced meaningful improvement.
Early assessment leads to faster, more straightforward recovery. The longer lateral elbow tendinopathy is left unaddressed, the more established the tendon changes tend to become.
Book an assessment
If you are unsure whether your symptoms represent tennis elbow, or if you have been managing elbow pain for some time without improvement, a single assessment is usually sufficient to give you a clear diagnosis and a structured plan for recovery.
We see patients at our Esher (KT10) and Southwark (SE1) clinics — including access to our private rehabilitation gym at Southwark for patients requiring supervised progressive loading. We also cover Claygate, Thames Ditton, Cobham, and Weybridge. Call 020 7193 9928 or visit vitality-physio.co.uk to book.

 Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy
Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy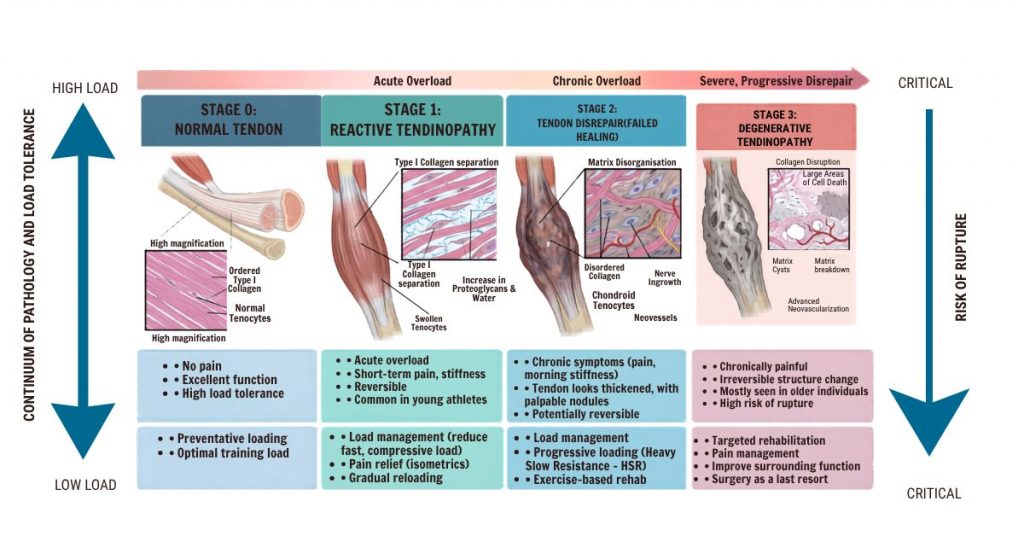


 At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
 We don’t have a house exercise for back pain. What we have is a framework: assess the whole person, understand their presentation (how irritable is the pain? what are their goals? what does their daily life look like?), and design a programme that introduces load progressively, builds capacity over time, and adapts as they improve.
We don’t have a house exercise for back pain. What we have is a framework: assess the whole person, understand their presentation (how irritable is the pain? what are their goals? what does their daily life look like?), and design a programme that introduces load progressively, builds capacity over time, and adapts as they improve.
 PEACE — The Early Phase
PEACE — The Early Phase Once the acute phase settles, the LOVE principles guide the return to full function:
Once the acute phase settles, the LOVE principles guide the return to full function:
 Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.
Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.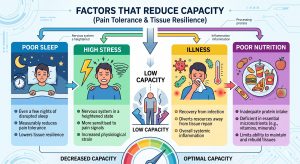 The factors that reduce capacity include:
The factors that reduce capacity include:



 Q1 When should I start pelvic floor exercises after birth?
Q1 When should I start pelvic floor exercises after birth? The term ‘Mummy MOT’ has become widely used, but it’s worth understanding exactly what it involves — and why it’s so valuable.
The term ‘Mummy MOT’ has become widely used, but it’s worth understanding exactly what it involves — and why it’s so valuable. Q4 How do I close a tummy gap (diastasis recti)?
Q4 How do I close a tummy gap (diastasis recti)? Q5 Is it safe to run after having a baby?
Q5 Is it safe to run after having a baby?