
Frozen Shoulder and Menopause: What Every Woman Over 40 Should Know
By Sangita Patel Associate Physiotherapist
If you’re a woman in your late forties or fifties and your shoulder has quietly gone from “a bit stiff” to “I can’t do my bra up or reach the top shelf,” you are not alone, and you are not imagining it. Frozen shoulder is one of the most misunderstood conditions we see in clinic, and it has a strong, under-discussed link to the hormonal changes of perimenopause. This article explains what’s actually happening in your shoulder, why this stage of life makes you more vulnerable, and what genuinely helps at each phase of the condition.
What Frozen Shoulder Actually Is
Let’s clear up the biggest myth first: frozen shoulder is not “wear and tear,” and it is not the same thing as a rotator cuff problem.
Frozen shoulder, medically known as adhesive capsulitis, is an inflammatory and fibrotic condition of the joint capsule, the fibrous envelope that surrounds your shoulder joint. In a healthy shoulder, this capsule is loose and stretchy, allowing a huge range of movement. In frozen shoulder, the capsule becomes inflamed, thickens, and forms adhesions (bands of scar-like tissue) that physically bind the joint down. The result is mechanical restriction, not just pain inhibiting movement.
What’s the difference between a Frozen Shoulder and Rotator Cuff problems?
This is a completely different process from rotator cuff tendinopathy or tears, which involve the tendons that move the shoulder rather than the capsule that contains it. Rotator cuff problems tend to cause pain with specific movements and weakness, but the passive range of motion (someone else moving your arm for you) is usually preserved. In frozen shoulder, even passive movement is blocked, because the capsule itself has physically tightened. This distinction matters enormously for diagnosis and treatment, and it is often where things go wrong when frozen shoulder gets treated like a simple rotator cuff strain.
Who Gets It, and Why
Frozen shoulder typically affects people between 40 and 60 years old, and women are affected considerably more often than men. Several well-established risk factors increase the likelihood of developing it:
- Diabetes (type 1 and type 2), where the risk is significantly higher, likely related to changes in collagen structure
- Thyroid disorders, both underactive and overactive
- A period of shoulder immobilisation, such as after surgery, a fracture, or a stroke, where the shoulder simply isn’t moved through its full range for a stretch of time
- Other autoimmune and inflammatory conditions
Here is the piece that gets far too little attention in most UK physiotherapy resources: the perimenopause connection.
How do declining hormone levels affect the shoulder?
Researchers have identified oestrogen receptors in the connective tissue of the shoulder capsule, and there is a growing, though still developing, body of research looking at how fluctuating and declining oestrogen through perimenopause might affect collagen quality and inflammatory response in this tissue. It is not yet fully settled science, but it offers a credible biological explanation for why frozen shoulder clusters so heavily in women in their late forties and fifties, often appearing alongside other perimenopausal symptoms such as joint aches, disrupted sleep, and broader changes in tendon and ligament resilience. Many women tell us their shoulder symptoms started around the same time as other perimenopausal changes, and while correlation isn’t proof, it is a pattern worth taking seriously rather than dismissing as coincidence.
A question we’re often asked is whether HRT changes the picture, either for risk or for recovery. At present, the research specifically looking at HRT and frozen shoulder is limited, and we can’t say with confidence that it prevents or speeds recovery from frozen shoulder itself. What we can say is that HRT is an important, separate conversation about your broader joint, tendon, and connective tissue health through perimenopause and menopause, and it’s worth raising with your GP or menopause specialist alongside anything we discuss about your shoulder.
This connection matters because it means frozen shoulder in this age group deserves to be assessed as part of a bigger picture, alongside your broader hormonal health, rather than treated as an isolated joint issue.
The Three Stages: Freezing, Frozen, Thawing
One of the most important things we can do for you is be honest about the natural course of this condition. Frozen shoulder typically moves through three stages:
Freezing stage (roughly 2 to 9 months). Pain is the dominant feature here, often worse at night and disturbing sleep. Movement gradually becomes more restricted as the capsule inflames and tightens.
Frozen stage (roughly 4 to 12 months). Pain often settles somewhat, but stiffness is now the main problem. Reaching, dressing, and sleeping on the affected side remain difficult because the range of movement is genuinely limited.
Thawing stage (roughly 6 to 24 months, sometimes longer). The capsule gradually loosens and movement slowly returns, often frustratingly slowly.
Put together, the full natural history can run anywhere from 12 to 30 months, occasionally longer. We tell patients this plainly because it builds trust rather than losing it. Nobody benefits from being told “this will settle in a few weeks” only to still be struggling a year later wondering what went wrong. Understanding the timeline helps you set realistic expectations, stay engaged with the right treatment at the right time, and recognise that slow progress is not the same as no progress.
How We Diagnose It
Frozen shoulder has a hallmark sign: loss of external rotation, meaning the movement of rotating your arm outward away from your body, with your elbow tucked in. This restriction is present with both active movement (you moving your own arm) and passive movement (someone else moving it for you), which is what points us away from a pure rotator cuff issue and toward the capsule itself.
A thorough assessment involves ruling out other conditions that can mimic frozen shoulder or coexist with it, including:
Rotator cuff tendinopathy or tears, which typically preserve passive range of motion
Glenohumeral osteoarthritis, which often shows a different pattern of restriction and may need imaging to confirm
Occasionally, more serious mimics, such as referred pain from the cervical spine or, rarely, other pathology that needs onward referral
Where the diagnosis is unclear, or the presentation is atypical, imaging such as X-ray or ultrasound may be used to rule out arthritis or a significant cuff tear before committing to a frozen shoulder treatment pathway. Getting this diagnostic step right at the start avoids months of the wrong treatment.
What Actually Helps, Stage by Stage
Good management can make a real difference to your function and your sleep, even though it can’t dramatically shorten the total timeline. The evidence points to different priorities at different stages.

In the freezing stage, when pain dominates, a corticosteroid injection into the joint is one of the most evidence-led interventions. Injections tend to be most effective when given early in this painful phase, reducing inflammation and pain significantly, which in turn allows better sleep and makes early, gentle physiotherapy more tolerable. Physiotherapy at this stage should focus on pain management, range-of-movement work within comfortable limits, and education, not aggressive stretching.
In the frozen stage, once acute inflammation has settled, physiotherapy shifts toward carefully progressed mobility work, targeted stretching, and strengthening to prevent the surrounding muscles from weakening through disuse. The emphasis is on working with the tissue’s current tolerance, gradually pushing range without provoking a flare.
For patients with persistent stiffness, hydrodilatation (also called distension arthrography) can be a useful option. Fluid is injected into the joint capsule under imaging guidance to stretch it from the inside. This is a useful option for patients with persistent stiffness, particularly those moving from the frozen into the thawing stage, who need an extra push to regain range.
In the thawing stage physiotherapy focuses on restoring full function, addressing any residual muscle imbalances, and returning to normal activities and exercise.
Throughout all of this “just wait it out” undersells what good management can achieve. Left entirely untreated, most people do eventually regain a functional range of movement, but they often do so with more pain, worse sleep, longer disability and sometimes a residual restriction. Matched, staged treatment doesn’t necessarily shorten the biological timeline of the capsule healing, but it dramatically improves how well you sleep, function, and cope while your shoulder works through it.
What Doesn’t Help
A few common approaches can genuinely make things worse or slow recovery:
Aggressive stretching too early, particularly during the freezing stage, tends to provoke more pain and inflammation rather than improving range. The tissue simply isn’t ready for it, and forcing movement can prolong the painful phase.
Generic exercise sheets handed out without proper assessment of which stage you’re in, often contain exactly the wrong exercises for where you currently are. A stretch that’s appropriate in the thawing stage can be counterproductive in the freezing stage.
Prolonged rest, on the other hand, allows the capsule to stiffen further and surrounding muscles to weaken, making eventual recovery harder. The goal is neither aggressive pushing nor complete avoidance, but calibrated movement matched to where your shoulder actually is.
Why it’s worth booking in with a women’s health physio

Frozen shoulder is a real, diagnosable condition — and one that disproportionately affects women in the perimenopausal years. That makes it worth assessing alongside your broader hormonal health, not in isolation.
A first appointment at our Southwark or Esher clinic with a women’s health physio gives you more than a shoulder assessment. As part of a thorough examination, we’ll rule out the other conditions that can look similar, such as rotator cuff pathology or osteoarthritis, and check carefully for anything that would need onward referral before we settle on a diagnosis, so you can move forward with confidence that nothing has been missed. Because we work specifically with women through perimenopause and menopause, we’ll also look at your shoulder in the context of the wider hormonal picture, rather than treating it as an isolated joint problem. That means a treatment plan built around which stage your shoulder is actually in, honest guidance on what to expect over the coming months, and a clear view on whether an injection, hands-on physiotherapy, or hydrodilatation is the right next step for you – all with ongoing support as you move through the freezing, frozen, and thawing stages.
If your shoulder has been getting stiffer and more painful over recent months, particularly if you’re also noticing other perimenopausal changes, it’s worth getting it properly assessed rather than assuming it will simply work itself out. Book an appointment with one of our women’s health physios and let’s get you a clear answer and a plan.

 Tennis elbow — clinically known as lateral elbow tendinopathy — is a condition affecting the tendons that attach the forearm extensor muscles to the outer elbow. The tendon most commonly involved is the extensor carpi radialis brevis (ECRB), which plays a central role in controlling wrist and hand movement.
Tennis elbow — clinically known as lateral elbow tendinopathy — is a condition affecting the tendons that attach the forearm extensor muscles to the outer elbow. The tendon most commonly involved is the extensor carpi radialis brevis (ECRB), which plays a central role in controlling wrist and hand movement.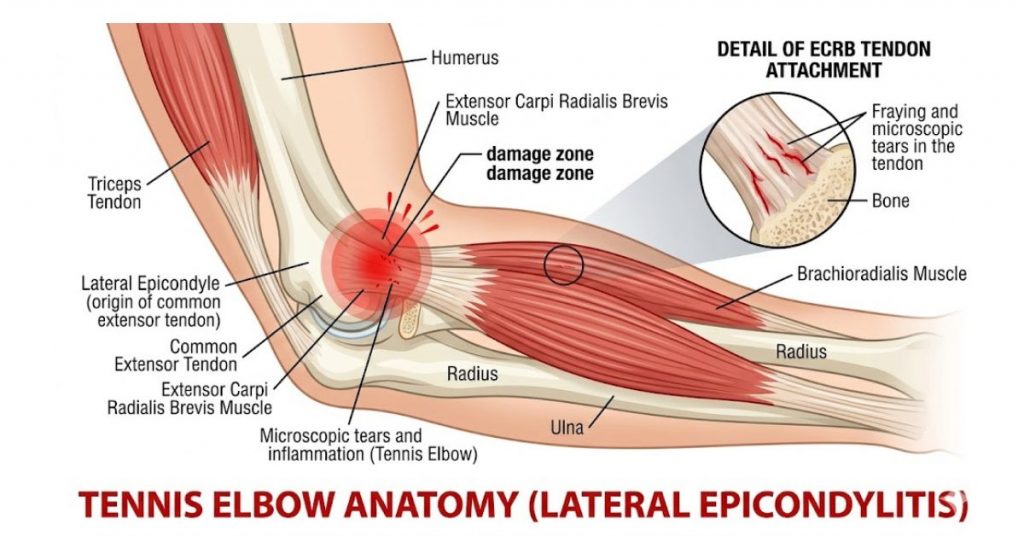

 Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy
Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy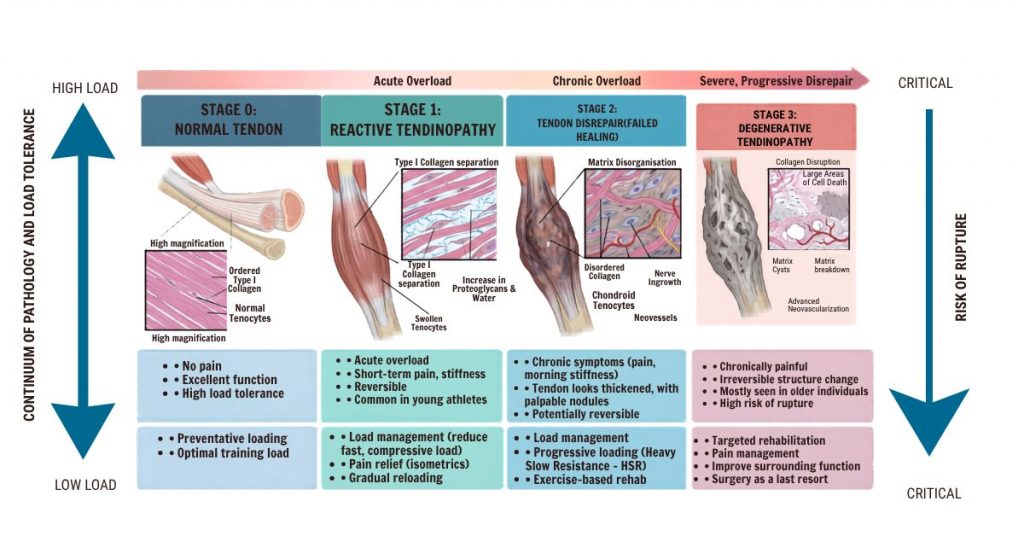


 At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
 We don’t have a house exercise for back pain. What we have is a framework: assess the whole person, understand their presentation (how irritable is the pain? what are their goals? what does their daily life look like?), and design a programme that introduces load progressively, builds capacity over time, and adapts as they improve.
We don’t have a house exercise for back pain. What we have is a framework: assess the whole person, understand their presentation (how irritable is the pain? what are their goals? what does their daily life look like?), and design a programme that introduces load progressively, builds capacity over time, and adapts as they improve.
 PEACE — The Early Phase
PEACE — The Early Phase Once the acute phase settles, the LOVE principles guide the return to full function:
Once the acute phase settles, the LOVE principles guide the return to full function:
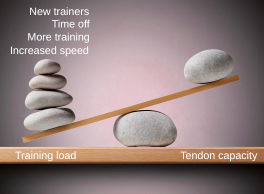
 Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.
Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.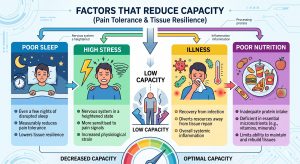 The factors that reduce capacity include:
The factors that reduce capacity include:


 How can tight pelvic floor muscles cause so many different symptoms?
How can tight pelvic floor muscles cause so many different symptoms? Treatment typically includes:
Treatment typically includes:
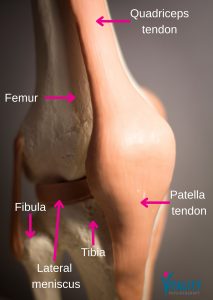
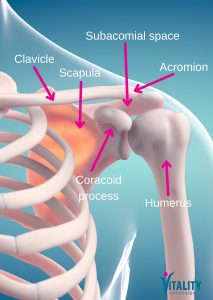 The shoulder is a remarkably mobile joint — but that mobility comes at a cost. A small space called the subacromial space runs between the top of the upper arm bone (humerus) and a bony arch formed by the shoulder blade (the acromion). Running through this space are the tendons of the rotator cuff and a small fluid-filled cushion called the subacromial bursa.
The shoulder is a remarkably mobile joint — but that mobility comes at a cost. A small space called the subacromial space runs between the top of the upper arm bone (humerus) and a bony arch formed by the shoulder blade (the acromion). Running through this space are the tendons of the rotator cuff and a small fluid-filled cushion called the subacromial bursa. Structural factors
Structural factors Recovery time varies depending on the severity of the impingement and any underlying structural changes. Most people with subacromial impingement see significant improvement within 6–12 weeks of consistent physiotherapy. Those with a concurrent partial rotator cuff tear, significant structural changes, or a longer history of symptoms may take longer.
Recovery time varies depending on the severity of the impingement and any underlying structural changes. Most people with subacromial impingement see significant improvement within 6–12 weeks of consistent physiotherapy. Those with a concurrent partial rotator cuff tear, significant structural changes, or a longer history of symptoms may take longer.