
Running Injuries: A Physiotherapist’s Complete Guide to Treatment, Recovery and Prevention
Expert guidance from Janine Enoch Founder of Vitality Physiotherapy — passionately working with runners across Surrey, Esher KT10, Cobham, Claygate, Weybridge, Woking and London SE1
Running is one of the most accessible, effective and rewarding forms of exercise — and around Esher and the wider Surrey area, it’s everywhere. From the wooded trails around Claygate and Oxshott to the towpath along the Thames near Weybridge, from Saturday morning parkruns to the Esher 10K, our community runs. And when injury strikes, it can feel devastating.
At Vitality Physiotherapy, with clinics in Esher (KT10) and Southwark (SE1), we work with runners at every level — from those lacing up for the first time to experienced athletes managing complex, recurring problems. This guide draws on over 25 years of clinical experience to help you understand the most common running injuries, why they happen, and what you can do about them.
Whether you’re dealing with knee pain that won’t shift, Achilles trouble that flares every time you build mileage, or you’re simply trying to stay injury-free as you train for your next event — this is written for you.
Who this guide is for: Recreational runners, parkrunners, half and full marathon trainers, returning runners after injury or a break, and anyone who wants to understand their body better.
Why Running Injuries Are So Common
Running is a high-load, repetitive activity. With every stride, your body absorbs force equivalent to two to three times your body weight — multiplied thousands of times over the course of a run. Most of the time, your body adapts beautifully to this. But when load exceeds your body’s capacity to absorb it, tissue becomes stressed and injury follows.
Research consistently shows that around 50–80% of runners experience at least one injury per year. The good news is that the vast majority of running injuries are not serious, are not caused by running itself, and respond well to physiotherapy — often without needing to stop running entirely.
The most common causes of running injury
- Too much, too soon — increasing mileage or intensity faster than the body can adapt
- Muscle weakness — particularly in the hips, glutes and core, which stabilise every stride
- Previous injury — undertreated or incompletely rehabilitated injuries are a major risk factor
- Training error — ignoring recovery, skipping rest days, or ramping up before a race
- Footwear — worn-out shoes, or shoes that don’t suit your gait pattern
- Biomechanical factors — how you run influences where load accumulates
A note from our clinic: In our experience at Vitality Physiotherapy, most running injuries we see in Surrey and London are not caused by bad luck — they are caused by identifiable, addressable factors. Understanding yours is the starting point for getting better.
The Most Common Running Injuries — and What to Do About Them
Below are the injuries we most frequently assess and treat at our Esher and Southwark clinics. Click the links to read our full articles on each condition.
- Runner’s Knee (Patellofemoral Pain Syndrome)
A dull ache at the front of the knee, often worse going downstairs or after sitting for long periods. Runner’s knee is one of the most common presentations we see, particularly in recreational runners who have recently increased their mileage.
It is frequently associated with hip weakness — when the glutes and hip abductors are not working effectively, the knee is forced to compensate, increasing load on the patellofemoral joint. Treatment focuses on load management, hip and quadriceps strengthening, and gradual return to full training.
Key message: Runner’s knee is not a reason to stop running permanently. With the right rehabilitation, most people return to full training.
- IT Band Syndrome
Sharp or burning pain on the outside of the knee, typically coming on at a predictable point in the run — often around the 2–3 mile mark. IT band syndrome is notoriously frustrating because it tends to recur when runners return too quickly or rely solely on foam rolling and stretching.
The IT band itself is not the problem — it is a symptom of a loading issue elsewhere, most commonly weakness in the hip abductors and poor pelvic control. Addressing these root causes, combined with a structured return-to-run programme, produces lasting results.
- Achilles Tendinopathy
Stiffness and pain at the back of the ankle, typically worst first thing in the morning or at the start of a run. Achilles tendinopathy is an overuse condition that requires careful load management — complete rest often makes things worse, not better.
Tendon rehabilitation is a speciality area at Vitality Physiotherapy. Evidence-based eccentric and progressive loading programmes, delivered consistently over time, are the most effective treatment. Most cases resolve fully with appropriate physiotherapy.
Important: If you have sharp pain or sudden onset swelling at the Achilles, seek assessment promptly — a tendon rupture requires different management entirely.
- Shin Splints (Medial Tibial Stress Syndrome)
Pain along the inner edge of the shin, usually diffuse and aching during and after runs. Shin splints are extremely common in newer runners and those returning after a break, and typically respond well to relative rest, load management and strength work.
Ignored or pushed through repeatedly, medial tibial stress syndrome can progress to a stress fracture — which requires a significantly longer recovery. Early assessment is important.
- Plantar Fasciitis
Stabbing pain in the heel, classically worst with the first steps in the morning. Plantar fasciitis is a loading issue affecting the connective tissue of the sole of the foot, and is influenced by calf tightness, foot biomechanics, and training load.
Treatment is effective but requires patience — this is an injury that responds to progressive loading rather than rest alone. Physiotherapy including calf and foot strengthening, load management advice, and where appropriate orthotic assessment produces excellent long-term outcomes.
- Hip and Glute Pain
Pain in the hip, buttock or outer thigh is increasingly common in recreational runners, particularly as we age or increase training demands. Presentations we see regularly include greater trochanteric pain syndrome (outer hip pain), hip flexor tendinopathy, and piriformis-related gluteal pain.
Many of these respond well to targeted strengthening and load management. If you have hip pain that radiates down the leg, a physiotherapy assessment is particularly important to identify the source accurately.
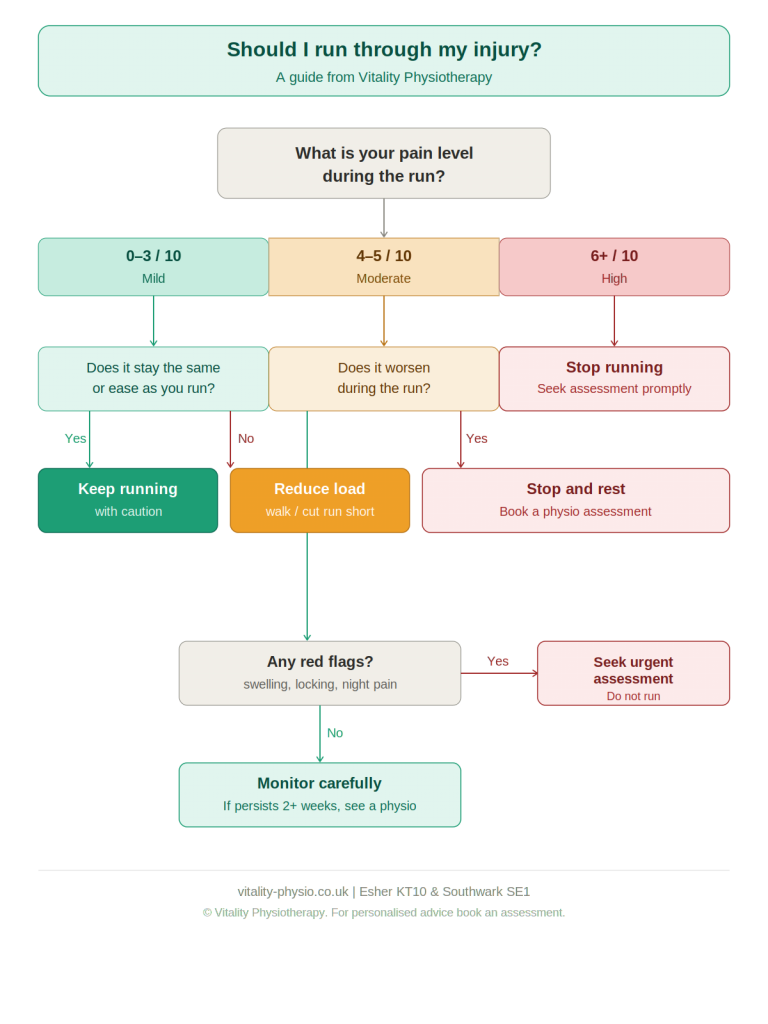
Should I Run Through an Injury?
This is the question we’re asked most often — and the honest answer is: it depends.
Some injuries can be managed while continuing to run at a reduced level. Others require a period of relative rest to allow the tissue to recover before loading resumes. The key factors are the type of injury, the severity of symptoms, and whether running is causing lasting damage or simply discomfort.
As a general guide:
- Pain above a 3 or 4 out of 10 during a run is a signal to reduce load or stop
- Pain that worsens significantly during a run, or that you are unable to run through, needs assessment
- Pain that is present at rest, especially at night, should always be assessed
- Swelling, giving way, locking, or sudden-onset sharp pain are red flags — seek assessment promptly
At Vitality Physiotherapy, we aim to keep you running wherever it is safe to do so. We work with you to find a manageable training level, modify your programme, and build back gradually — rather than telling you to stop until everything is perfect.
Running Injury Prevention: What the Evidence Says
The single most effective thing you can do to reduce your injury risk as a runner is strength training. A growing body of research demonstrates that runners who include regular strength work — particularly targeting the hips, glutes and single-leg stability — sustain fewer injuries and recover faster when they do.
Beyond strength work, the evidence supports:
- Gradual load progression — the commonly cited ‘10% rule’ is a useful starting point
- Adequate recovery — rest days are not optional; they are when adaptation happens
- Sleep — consistently underrated as an injury risk factor
- Appropriate footwear — not necessarily the most expensive, but suited to your foot type and gait
- Addressing previous injuries properly — incomplete rehabilitation is one of the strongest predictors of future injury
From our clinic: We often see runners who have been managing a ‘niggle’ for months before seeking help. Early physiotherapy assessment — before a minor issue becomes a significant injury — is almost always the better approach.
When to See a Physiotherapist
You do not need to wait until you cannot run to seek physiotherapy. The following are all good reasons to book an assessment:
- A pain or ache that has persisted for more than 2 weeks
- An injury that keeps coming back in the same location
- Pain that is changing how you run — altering your gait or causing you to compensate
- You are training for an event and want to manage a problem before it escalates
- You want a running assessment to identify any biomechanical factors that may be increasing your injury risk
At Vitality Physiotherapy, our running assessments are carried out by experienced chartered physiotherapists who understand both the clinical and training demands of running. We do not offer one-size-fits-all advice — every runner is different, and every treatment plan is individual.
Running Physiotherapy in Surrey and London — Our Clinics
Vitality Physiotherapy has two clinic locations:

Esher, Surrey (KT10)
Our Surrey clinic is conveniently located for runners across Esher, Claygate, Cobham, Oxshott, Hersham, Hinchley Wood, Thames Ditton and Weybridge. We are a short walk from Esher station on the South Western Main Line.
We regularly see runners preparing for local events including the Esher 10K, the Claygate 5K, and a range of half and full marathons across Surrey and London.
Southwark, London (SE1)
Our London clinic is located in Southwark SE1, close to London Bridge station. We see runners from across South and Central London, including those training for the London Marathon, the Big Half, and the many parkruns across the capital.
Both clinics offer the full range of physiotherapy services including running assessments, injury rehabilitation, and women’s health physiotherapy — our specialist area of practice for over 25 years.
Book a Running Assessment
If you are dealing with a running injury, managing a recurring problem, or simply want an expert assessment of your running health, we would love to help.
Book online at vitality-physio.co.uk or call us to speak with a member of the team.
Esher KT10 | Southwark SE1 | vitality-physio.co.uk
Pelvic floor issues when you run? Read this

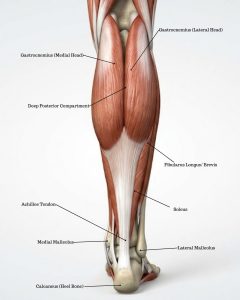 The Achilles tendon is the largest and strongest tendon in the body. It connects the calf muscle complex — the gastrocnemius (medial and lateral heads) and soleus — to the heel bone (calcaneus), forming a thick, powerful structure that stores and releases energy with every step. It is central to walking, running, jumping, and pushing off the foot.
The Achilles tendon is the largest and strongest tendon in the body. It connects the calf muscle complex — the gastrocnemius (medial and lateral heads) and soleus — to the heel bone (calcaneus), forming a thick, powerful structure that stores and releases energy with every step. It is central to walking, running, jumping, and pushing off the foot. Load management The first step is to reduce aggravating activities to a level the tendon can tolerate, while maintaining as much training as possible. Complete rest is rarely helpful and may slow recovery.
Load management The first step is to reduce aggravating activities to a level the tendon can tolerate, while maintaining as much training as possible. Complete rest is rarely helpful and may slow recovery.