Patellar Tendinopathy “Jumper’s Knee” Understanding Pain Below the Kneecap
That nagging ache just below the kneecap. The stiffness at the bottom of the stairs in the morning. The way it flares after a hard session and lingers for days. If this sounds familiar, you may be dealing with patellar tendinopathy — one of the most common overuse injuries we see at Vitality Physio.
Also known as ‘jumper’s knee’, patellar tendinopathy affects the tendon just below the kneecap and is especially prevalent in sports that demand explosive, repetitive effort: football, rugby, basketball, volleyball, netball, and athletics. But you don’t need to be an elite athlete to develop it. Recreational gym-goers, runners, and anyone who has ramped up their training too quickly can find themselves dealing with the same persistent, frustrating symptoms.
The good news — and it is genuinely good news — is that patellar tendinopathy responds very well to the right approach. Not rest, not waiting it out, but a progressive rehabilitation programme built around gradually rebuilding what the tendon can handle. With the right guidance, most people return fully to the sport and training they love.
What Is Patellar Tendinopathy?
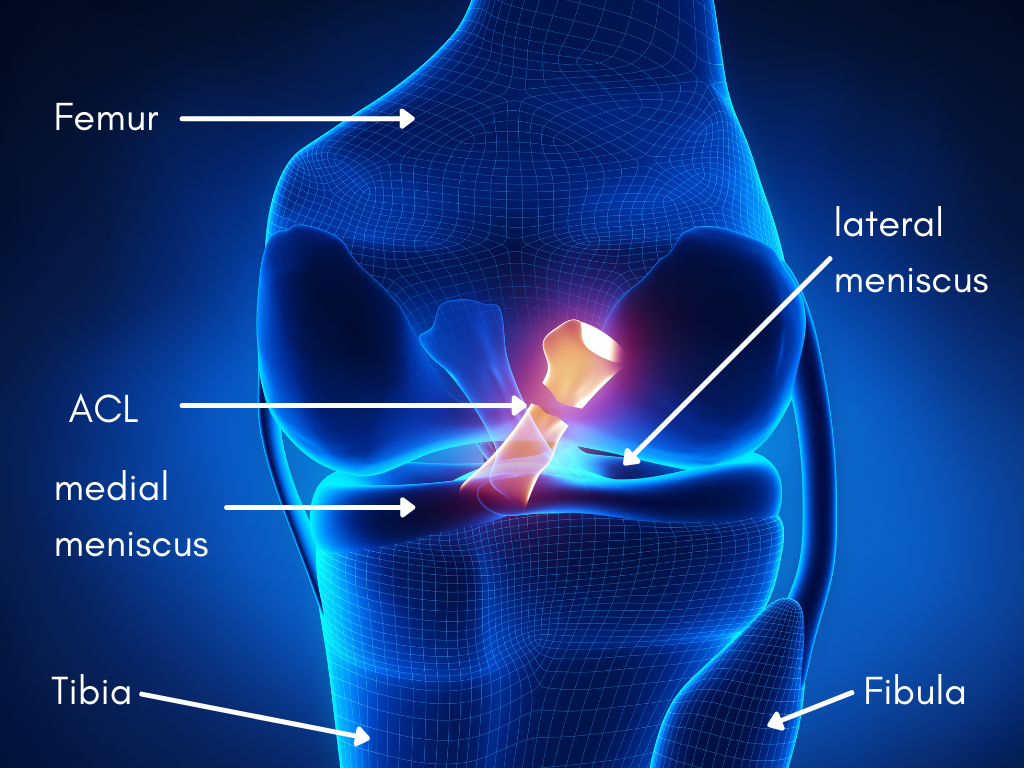
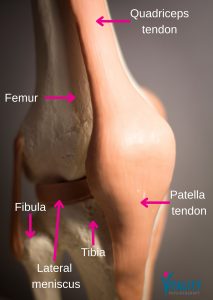
The patellar tendon connects the kneecap (patella) to the shin bone (tibia). It plays a central role in virtually everything that involves the knee: running, jumping, squatting, kicking, and landing.
Patellar tendinopathy develops when the tendon is repeatedly overloaded without sufficient recovery. Over time, the tissue becomes irritated and painful — particularly at the attachment point just beneath the kneecap.
Importantly, this is not simply an inflammatory problem. It is better understood as a tendon overload condition: the demands placed on the tendon have outpaced its current capacity. Understanding this distinction matters, because it shapes everything about how we rehabilitate it.
Common Symptoms
- People with patellar tendinopathy typically describe:
- Pain directly below the kneecap
- Discomfort during jumping, sprinting, or explosive movements
- Aching with squatting or lunging
- Stiffness at the start of a session that eases as the tendon warms up
- Symptoms that return after exercise — often later the same day or the following morning
- Localised tenderness when pressing on the tendon
Symptoms often fluctuate in line with training load and sporting demand. Unlike many ligament injuries, patellar tendinopathy is not typically associated with significant swelling, locking, or instability of the knee.
Why Does It Develop?
The most common trigger is a sudden spike in the load placed through the tendon. This can take many forms:
- A sharp increase in training intensity or frequency
- Significantly more jumping or sprinting than usual
- Returning to sport too quickly after time off
- Playing multiple matches or tournaments in a short window
- Changes in training surface, footwear, or technique
- Rapid increases in gym-based loading — particularly heavy squats or leg press
A number of physical factors can also increase vulnerability, including:
- Quadriceps weakness
- Reduced calf strength and ankle mobility
- Poor landing mechanics or running patterns
- Hip and core weakness
- Inadequate recovery between training sessions
In many cases the tendon itself is not ‘damaged’ in the traditional sense — it is simply being asked to cope with more than it currently has the capacity for.
Who Is Commonly Affected?
Patellar tendinopathy is most prevalent in sports involving repeated explosive movements, but it crosses all levels of participation:
- Football and rugby players
- Basketball and volleyball athletes
- Netball players
- Sprinters and field athletes
- Gym-based athletes, particularly those focused on strength and power
- Recreational runners
- Adolescents and young adults carrying high training volumes
It is especially common during periods of increased sporting demand, condensed competition schedules, or when returning after a break.
How Is Patellar Tendinopathy Diagnosed?
Diagnosis is primarily clinical — based on a careful, detailed assessment rather than imaging alone. At Vitality Physio, our assessment examines:
- The precise location and behaviour of symptoms
- Tendon tenderness on palpation
- How symptoms respond to loading during the session
- Your training history and any recent changes in load
- Lower limb strength and movement control
- Jumping and landing mechanics
- Hip, knee, and ankle function
Imaging such as ultrasound or MRI can provide useful supporting information, but it is rarely the deciding factor — many people with significant tendon changes on scan have no symptoms at all, and vice versa.
Does Rest Actually Help?
Complete rest is rarely the answer — and can sometimes make things worse.
While temporarily reducing the activities that aggravate symptoms makes sense in the short term, tendons respond far better to carefully graded loading than to prolonged inactivity. Extended rest reduces tendon capacity, making it even harder to return to sport when the time comes.
Our approach focuses on managing load intelligently while progressively rebuilding tendon strength. In practice, this often means:
- Temporarily reducing jumping and sprinting volume
- Modifying gym-based exercises
- Adjusting training intensity and frequency
- Maintaining activity within tolerable limits
- Gradually reintroducing explosive movements as capacity improves
| Pain Monitoring in Rehabilitation
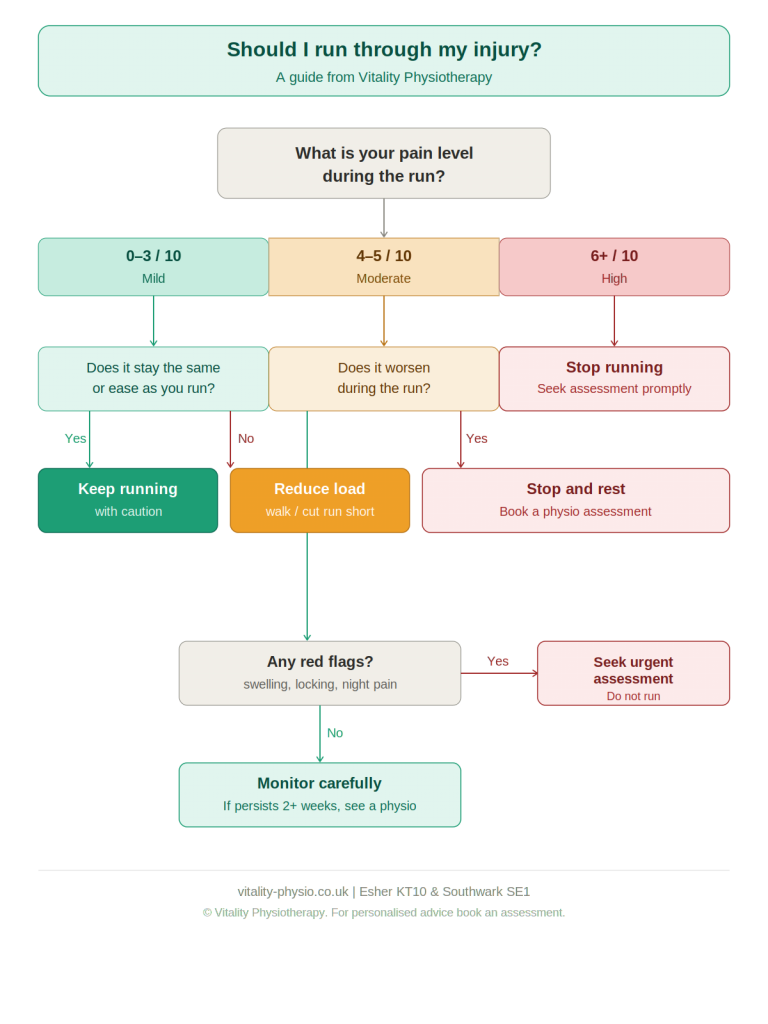
A useful guide during rehabilitation is the pain-monitoring model:
✔ Mild discomfort (≤ 4/10) during exercise is acceptable ✔ Symptoms should settle relatively quickly after activity ✔ Pain should not be significantly worse the following morning
If symptoms consistently flare beyond these parameters, load adjustment is likely needed. |
What Does Physiotherapy Treatment Involve?
 At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
At Vitality Physio, rehabilitation is built around improving the tendon’s load tolerance while addressing the contributing factors that drove the problem in the first place.
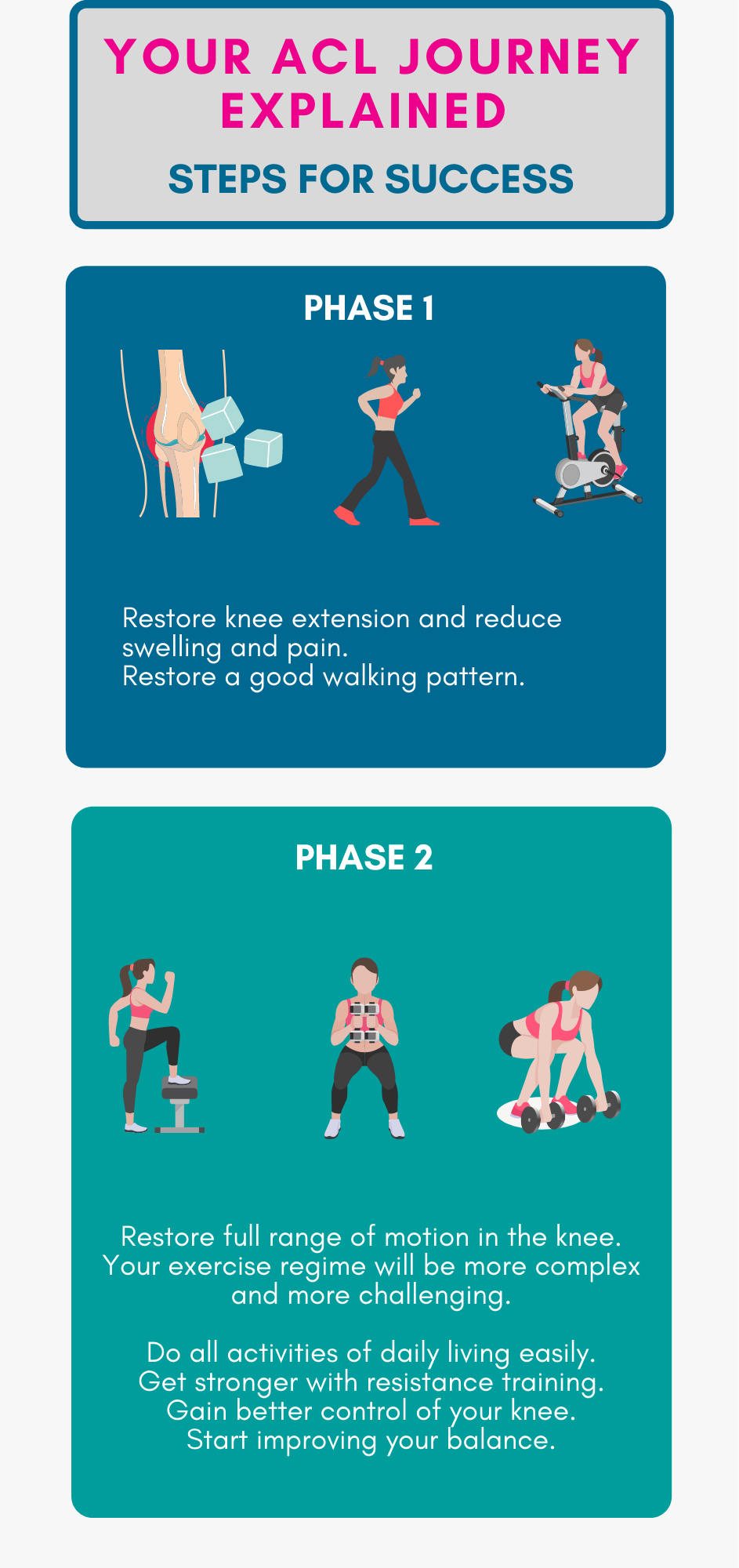
Progressive Tendon Loading
Exercise-based rehabilitation is the cornerstone of evidence-based tendon management. Programmes are structured to progress through distinct phases:
- Isometric exercises for initial pain management and tendon engagement
- Heavy slow resistance training to drive tendon adaptation
- Eccentric strengthening work
- Plyometric and energy-storage drills
- Return-to-sport loading progressions
The pace of progression is guided by your symptoms, strength levels, and the demands of your sport — not a fixed calendar.
Strength Rehabilitation
Targeted strengthening commonly focuses on:
- Quadriceps strength and capacity
- Glute and hip stability
- Calf strength and load absorption
- Core control
Building robust lower limb strength reduces the stress concentration through the patellar tendon during sport and training.
Movement Retraining
Where poor landing mechanics, running patterns, or jumping technique are contributing to tendon overload, we address these directly — making them part of the rehabilitation process rather than an afterthought.
Load Management
Understanding how to balance training, competition, and recovery is one of the most important — and often most overlooked — aspects of tendon rehabilitation. We work with you on practical load management strategies to reduce the risk of recurrence.
Common Rehabilitation Mistakes
Patellar tendinopathy frequently becomes persistent when rehabilitation is managed incorrectly. The most common pitfalls include:
- Resting completely for prolonged periods — reducing tendon capacity further
- Returning to jumping or explosive work too early in the process
- Progressing plyometrics too aggressively before adequate strength is in place
- Ignoring underlying strength deficits
- Training through significant pain
- Neglecting load management outside of physiotherapy sessions
Successful tendon rehabilitation takes patience and consistency. The good news is that with the right approach, the outcomes are genuinely excellent.
How Long Does Recovery Take?
Patellar tendinopathy typically takes longer to resolve than people expect — often longer than a straightforward ligament sprain or muscle strain.
Most people notice meaningful improvement within 8–12 weeks of consistent rehabilitation. Full recovery — including return to unrestricted sport — can take several months, particularly if symptoms have been present for some time before treatment begins.
The people who recover best tend to share a few things in common: they stay consistent with their rehabilitation, progress loading gradually rather than rushing, avoid repeated flare-ups through sensible load management, and address the strength and movement factors that contributed to the problem in the first place.
When Should You Seek Physiotherapy?
We recommend a physiotherapy assessment if:
- Pain is limiting your sport, training, or exercise
- Symptoms have persisted for more than two to three weeks
- Jumping, running, or squatting is becoming increasingly painful
- You are experiencing repeated flare-ups with activity
- Symptoms are beginning to affect your performance or confidence
Please seek urgent medical assessment if:
- Symptoms followed a significant injury, fall, or trauma
- The knee has become notably swollen
- You are unable to bear weight through the leg
- The knee is locking or giving way repeatedly
How Vitality Physio Can Help
At Vitality Physio, we provide evidence-based assessment and rehabilitation for patellar tendinopathy and sports-related knee pain across our clinics in Southwark SE1 and Esher KT10.
Our approach combines thorough clinical assessment, progressive tendon loading, targeted strength rehabilitation, movement retraining, and practical load management — giving you both the tools and the understanding to return confidently to the sport and activity you love.
Early intervention generally leads to faster recovery and significantly reduces the risk of symptoms becoming persistent. If you are experiencing pain below the kneecap, we would be glad to help.
| Book an Assessment
Southwark SE1 | Esher KT10 vitality-physio.co.uk
|



 At Vitality Physiotherapy, our approach focuses on restoring the balance between load and tissue capacity — not simply resting the painful area and hoping for the best.
At Vitality Physiotherapy, our approach focuses on restoring the balance between load and tissue capacity — not simply resting the painful area and hoping for the best.