Most of us know someone in our social circles who has had COVID-19, with or without becoming sick from it.
Within the last 20 months, more than 203M cases of coronavirus infections were reported worldwide. Some people recovered from SARS-CoV-2 COVID having only a sniffle or a cough. Others got COVID and became sick with unremitting fever for days or even weeks. Sadly for 4.3 million people, this terrible disease was fatal.
It begs the question – why do some people get so sick from COVID, whilst others suffer just mild symptoms? Is it a case of genetics, age, sex, or previous co-morbidities?
This article aims to answer this question.
The journal Science Immunology published a study in March 2021 found that severe COVID-19 is accompanied by elevated levels of multiple inflammatory blood markers. It became apparent that a person’s immune response to SARS-CoV-2 determines who is at the greatest risk rather than the virus itself.
HOW DOES THE IMMUNE RESPONSE BEHAVE IN COVID-19?
In COVID-19, coronavirus particles spread across the respiratory tract and infect surrounding uninfected cells. This triggers a series of immune responses. It results in some changes in immune cells, particularly lymphocytes, which then leads to immune system dysfunction.
Cells of the immune system communicate with each other through a process known as signaling. Cells respond to viruses by secreting proteins called cytokines. However, in the presence of excessive inflammation, sometimes there is an uncontrolled release of cytokines. This triggers a ‘cytokine storm.’ The cytokines released by the SARS-COV2 infection lower white blood cells (such as lymphocytes) and suppress the immune response.
Some cytokines cause lung cells to die. As those lung cells break down and die, the alveoli (air sacs in your lungs) fill with fluid. This causes pneumonia and prevents the exchange of air in the lungs. The body becomes deprived of oxygen (hypoxia) and respiratory distress occurs.
Are you starting to understand why COVID makes some people so sick?
WHY IS COVID-19 SO MUCH MORE DANGEROUS IN OBESE AND OLDER AND VULNERABLE POPULATIONS?
1.OBESITY:
A recent study published in The Lancet Diabetes and Endocrinology analyzed COVID-19 severity in 6.9 million people in England. It demonstrated that a BMI over 23 kg/m2 was associated with an increased risk of severe COVID-19.
It has been suggested that obesity is associated with an inflammatory state. WE see a surplus of macronutrients in obesity fat tissues. The macronutrients cause increased production of inflammatory mediators (tumor necrosis factor* and interleukin-6) and reduce adiponectin. Adiponectin is a hormone that plays a crucial role in protecting against insulin resistance/diabetes. The result is oxidative stress and pro-inflammatory reaction. During oxidative stress, the body is overloaded with free radicals and not enough antioxidants
During normal metabolic processes, the body’s cells produce free radicals. The cells also produce antioxidants that neutralize these free radicals. In general, the body can maintain a balance between antioxidants and free radicals. An imbalance favoring free radicals causes oxidative stress.

Clinical manifestations and mechanisms for COVID-19 risk in individuals with obesity
Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obesity Reviews November 2020 e13128
Individuals with obesity are more likely to develop diabetes type 2. Hyperglycemia (excessive blood sugar), and uncontrolled blood glucose, have been shown to significantly impair immune cell function and was associated with a higher mortality rate.
A high-fat diet also triggers an inflammatory response in the body. The fatty acid, Cholesterol is an essential ingredient in the spread of SARS COV-2. This virus enters the cell in the presence of cholesterol in the form of lipid rafts, The virus attaches and enters the cell by being engulfed by the cell (endocytosis). An exciting discovery was recently discovered by the University of Birmingham, Keele University, and the San Raffaele Scientific Institute in Italy, where fenofibrate, a blood cholesterol-lowering drug, decreased sARS-COV-2 significantly in laboratory testing.
2. OLDER PEOPLE
Over 65-year-olds represent 80% of hospitalizations and have a 23-fold greater risk of death. Cardiovascular disease, diabetes, and obesity increase the risk of fatal disease, but they do not explain why age is an independent risk factor.
By 29 May, the Office for National Statistics reported that more than 46,000 people had died from Coronavirus in England and Wales, and that more than 4 in 5 of those people were over the age of 70. When we examine the number of deaths caused by Coronavirus per thousand people, the correlation is even starker.
In age groups up to and including 60-69, fewer than 1 in 1,000 people have died from coronavirus.
Age 70-79, is 2 in every 1,000 people.
Age 80-89, is 7 in every 1,000 people.
Age 90 and over, is 18 people in every 1,000 people.
 Una instantánea de la carrera mundial de vacunas dirigidas contra el SARS-CoV-2 y la pandemia COVID-19. Parte delantera. Pharmacol. 11:937.Funk CD, Laferrière C and Ardakani A (2020) A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic. Front. Pharmacol. 11:937.https://doi.org/10.3389/fphar.2020.00937, CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=99473789")
By Colin D. Funk, Craig Laferrière, and Ali Ardakani – Funk CD, Laferrière C y Ardakani A (2020) A (2020) A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic.
The virus typically enters an individual’s airways and enters a cell by attaching its spike protein to the ACE-receptors found on the surface of many organs in the body. The virus becomes engulfed by the the cell (endocytosis), and then begins to replicate, taking over and replicating itself using the body’s own protein making mechanism.
Two major changes occur in the immune system as we age. There is a gradual decline in immune function known as immunosenescence, which hampers pathogen recognition, alert signaling, and clearance of pathogens. Other classic immune system changes during aging are chronic inflammation and inflamaging, which result from an overactive, but ineffective alert system.
The virus continues replicating and spreading in the body, causing chaos and damage as it does.
The aging immune system
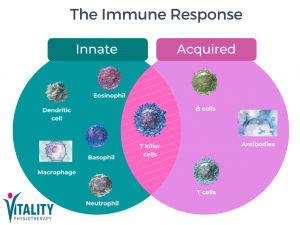
A patient’s ability to control viral load is one of the best predictors of whether they will become mildly or severely sick from COVID-19. The immune system requires four main functions: (1) recognise, (2) alert, (3) destroy, and (4) clear to destroy any virus. In older adults, each of these mechanisms is dysfunctional and increasingly variable. The immune system’s response is usually two-fold. Our first reaction relates to the innate immune response which is characterised by the cytokine and interleukin response, which serves to slow down the replication of the virus, and to allow the body to launch it is personal bespoke acquired immune response which seeks to destroy the virus. However, in older people where the immune workings are less than optimal and variable, the virus is by default is more opportunistic.

Image: The mechanism of the human immune response Source Cell Signaling Technology
OTHER HEALTH CONDITIONS:
Several health conditions, such as diabetes, can increase the risk of becoming severely sick from COVID-19 by suppressing the immune system; whilst COPD, increases the risk due to the weakened state of the lungs. This is largely due to poor underlying lung reserve (The amount of extra air inhaled — above normal shallow breathing when taking a forceful breath) as well and increased expression of angiotensin-converting enzyme 2 (ACE-2) receptor in the small airways
Increased risk has also been seen in people with high blood pressure (hypertension) and coronary artery disease. Fever and infection cause the heart rate to speed up, increasing the work of the heart in COVID-19 patients who develop pneumonia. Blood pressure may drop or spike, causing further stress on the heart, and the resulting increase in oxygen demand can lead to heart damage. This is especially so, if the heart arteries or muscle were unhealthy, to begin with. Heart damage is most often caused by heart attacks, which result from the formation of a blood clot in a vulnerable heart artery, blocking the delivery of oxygen to the heart muscle. COVID-19-related inflammation raises the risk of this type of heart attack by activating the body’s clotting system and disrupting the blood vessel lining. This lining loses its ability to resist clot formation when inflamed. Clots in the large and small arteries of the heart cut off the heart’s oxygen supply. The increased clotting tendency can also cause blood clots in the lungs, which can cause the oxygen level in the blood to drop. A severe case of pneumonia further reduces blood oxygen levels.
As previously described when the ‘spike’ molecule on the surface of the virus particle binds to ACE2 on the surface of a cell. This causes the virus particle to be taken into the cell. It replicates its genetic material to form new virus particles. Normally, cells in the airways, lungs, and heart, as well as those in the circulatory system, contain ACE2.
However, patients with heart failure or respiratory conditions like COPD have an increase in ACE2. A higher level of ACE2 means that there are more entry points for the virus and therefore increase the risk of severe illness. Please note that if you have been prescribed ACE inhibitors, you should continue taking them. ACE inhibitors and ARBs are safe to use.
The researchers at Kings College London found that there was no link between the use of angiotensin-converting enzyme (ACE) inhibitors, used to treat blood pressure or diabetes, and how sick you get from Covid-19.
“This study has addressed a very important clinical question since a large proportion of the UK population takes these cardiovascular drugs. Our study indicates that it is perfectly safe to continue taking these agents and that people’s concerns about them can be alleviated”
– Professor Ajay Shah, BHF Chair of Cardiology & James Black Professor of Medicine Director,
King’s BHF Centre of Excellence, King’s College London and King’s College Hospital
So, the older you are, the more health issues and underlying conditions that you may have, the more severe the risk of severe infection. However, taking the necessary steps to protect yourself and others from becoming sick with COVID-19, is possible.
Vaccination, social distancing, wearing a face covering, and practicing hand hygiene remain crucial to help reduce the spread of COVID-19.
If you would like to learn more about how physiotherapy can help you recover from Long-COVID, this article will answer all your questions!
If you are currently experiencing symptoms associated with COVID-19 or Long-COVID and would like to speak to an expert, get in touch: info@vitality-physio.co.uk












 Proposed Mechanism of how Long Covid causes fatigue by Vitality Physiotherapy
Proposed Mechanism of how Long Covid causes fatigue by Vitality Physiotherapy



 Una instantánea de la carrera mundial de vacunas dirigidas contra el SARS-CoV-2 y la pandemia COVID-19. Parte delantera. Pharmacol. 11:937.Funk CD, Laferrière C and Ardakani A (2020) A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic. Front. Pharmacol. 11:937.https://doi.org/10.3389/fphar.2020.00937, CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=99473789")