
Understanding Tendinopathy: Why Tendons Become Painful — And How to Get Them Strong Again
 Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy
Written by George Eaton, MSK Physiotherapist, Vitality Physiotherapy
As a physio who spends a good chunk of my own time in the gym, I’ve seen first-hand how frustrating a tendon injury can be. You’re in the middle of a solid training block — progress is happening, you’re feeling strong — and then a nagging pain in your Achilles, knee, or shoulder starts to creep in. You try to push through, rest it for a few days, maybe Google it… and you end up more confused than when you started.
The good news? Tendinopathy is one of the most treatable musculoskeletal conditions — when you understand what’s going on and approach it the right way. So let’s break it down.
What Is Tendinopathy?
A tendon is the tough, rope-like structure that connects your muscle to your bone. Its job is to transmit the force your muscle generates so you can move, jump, push, and pull. When working well, tendons are incredibly resilient — they absorb and release energy like a spring.
Tendinopathy is the umbrella term for a painful, dysfunctional tendon. It’s caused by an overload — where the load placed on the tendon consistently exceeds its capacity to recover.
You might have heard the old term ‘tendinitis,’ which implied the problem was inflammation. We now know the picture is more complex than that — and that understanding the actual pathology changes how we treat it.
Tendons commonly affected include:
- Achilles tendon (heel/calf area) — particularly in runners
- Patellar tendon (just below the kneecap) — common in jumping sports
- Gluteal tendons (outer hip) — frequently seen in women, especially around menopause
- Rotator cuff tendons (shoulder) — often in gym-goers and overhead athletes
- Hamstring tendons (sit-bone area) — particularly in distance runners
- Elbow tendons (lateral or medial epicondyle) — tennis or golfer’s elbow
What’s Actually Happening in the Tendon?
This is where things get interesting — and where a lot of online advice goes wrong.
Tendons don’t behave like other soft tissues. They have a poor blood supply and a slow metabolic rate, which means they adapt and heal more slowly than muscle. When a tendon is repeatedly overloaded, the collagen fibres — which normally run in neat, parallel lines — begin to disorganise. The tendon responds by producing more collagen, but it’s not the same high-quality collagen. Instead, you get a disorganised matrix, new (often painful) nerve ingrowth, and sometimes areas of degeneration within the tendon substance.
The Three Stages of Tendinopathy
Researchers have described a continuum of tendon pathology, which helps explain why some tendon pain responds quickly to treatment, while other cases are more stubborn:
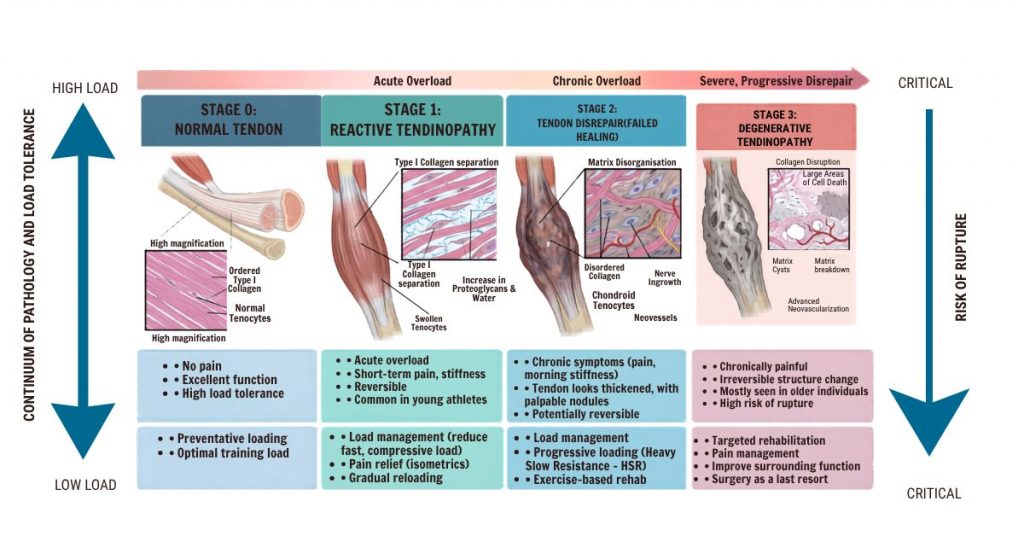
Stage 1: Reactive Tendinopathy
This is an early, acute response to overload. The tendon swells and becomes thickened, but the change is largely reversible at this stage. You’ve spiked your training too quickly, changed your footwear, or done something your tendon wasn’t ready for. Rest and load management can resolve this effectively.
Stage 2: Tendon Dysrepair
The tendon has tried to repair itself but is struggling. You start to see more disorganised collagen and some early cellular changes. The tendon isn’t in crisis, but it’s not healing cleanly either. This is where many people sit when they’ve had symptoms for several weeks to months.
Stage 3: Degenerative Tendinopathy
In more longstanding cases, areas of the tendon may become truly degenerative — with cell death, disrupted collagen architecture, and fatty or calcific deposits. Interestingly, the most degenerated areas of the tendon are often not the most painful. Pain in tendinopathy is complex and driven by nerve sensitisation as much as tissue damage.
Why Does It Hurt?
Tendon pain can be a confusing beast. Here are a few things that make it different from other injuries:
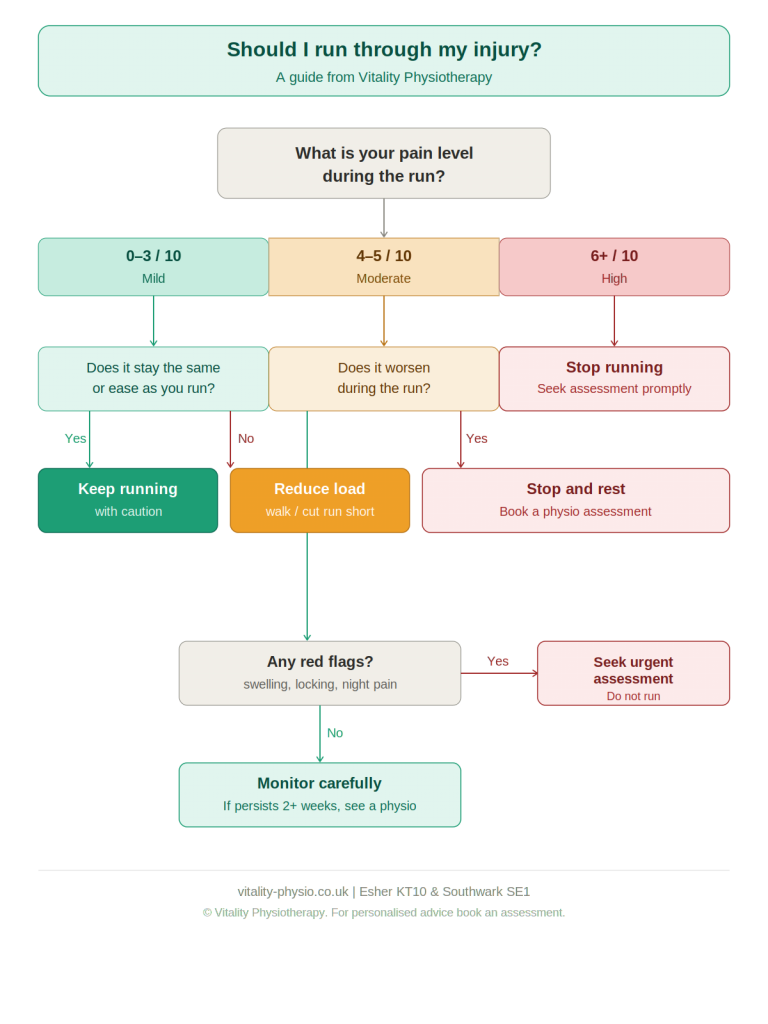
- It’s load-sensitive. Tendons love consistent, progressive loading — but hate sudden spikes. The pain is often provoked by activity and may ease once you warm up, only to return later.
- Morning stiffness is classic. Many people describe a stiff, achy tendon first thing in the morning that loosens off after a few minutes of movement.
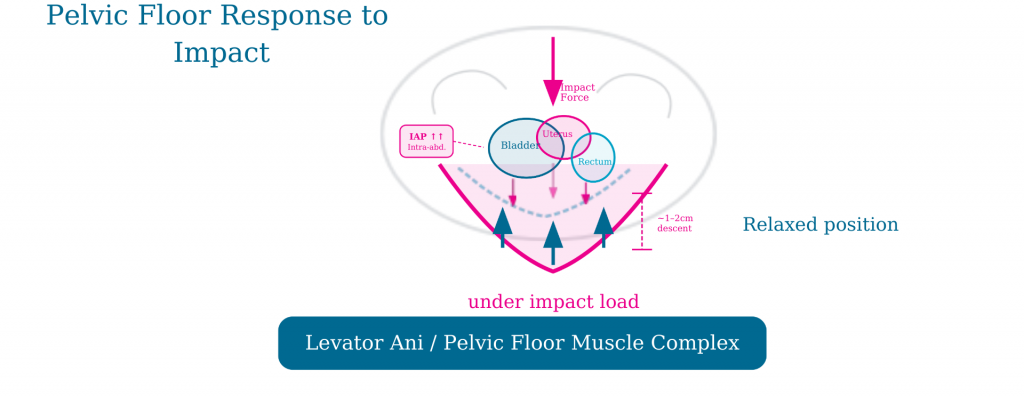
- Compressive loads can be particularly aggravating. Positions that compress the tendon against a bony surface — such as stretching a tendon under tension — can be more provocative than simple tension. This is especially relevant for Achilles and gluteal tendons.
- Pain doesn’t equal damage. The level of pain doesn’t reliably indicate how much structural damage is present. Some badly degenerated tendons are painless; some reactive tendons are extremely painful.
Treatment: What Actually Works
Let me be direct here: the evidence for tendinopathy management has moved on enormously in the past decade. Rest alone doesn’t fix tendons — in fact, complete rest weakens them further. What tendons need is the right kind of load, applied progressively and intelligently.
1. Load Management
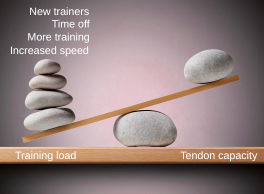
The first step is always to identify what has changed in your training or activity that caused the tendon to become overloaded. This might be a sudden increase in mileage, a return to sport after time off, new footwear, or a change in surface. We reduce the provocative load — not eliminate it entirely — and create a stable baseline from which to build.
2. Isometric Exercise: The Pain-Relieving Starting Point
Isometric contractions — where you contract the muscle without any movement — have been shown to reduce tendon pain quite quickly and are a great starting point. They provide load to the tendon without the compression or repeated movement that can aggravate it. For example, a wall sit for a patellar tendon, or a calf press held in a fixed position for the Achilles.
3. Heavy Slow Resistance Training
This is the cornerstone of tendinopathy rehabilitation. Research consistently shows that heavy, slow resistance training — where muscles and tendons are loaded through their full range in a slow, controlled manner — stimulates collagen remodelling and improves tendon structure over time.
This is exactly the kind of work I love in the gym environment. Exercises like heavy heel raises, leg press, hip thrusts, and cable pull-throughs can all be used therapeutically, depending on which tendon is affected. The key is progressive overload — we gradually increase the load as the tendon adapts.
4. Energy Storage and Return Loading
Once the tendon is tolerating slow, heavy load, we progress to exercises that challenge the tendon’s spring-like properties — things like hopping, bounding, and sport-specific movements. This phase is essential if you want to get back to running, jumping, or dynamic sport. Skipping it is one of the most common reasons people re-injure.
5. Addressing Contributing Factors
Tendinopathy rarely exists in isolation. We always assess the whole picture: hip strength and control, foot mechanics, training load patterns, sleep, nutrition, and for women in particular, hormonal status — oestrogen plays a significant role in tendon health, which is why gluteal and Achilles tendinopathy are especially common around perimenopause.
What to Avoid
A few things that commonly make tendinopathy worse — even though they seem logical:
- Complete rest: Tendons need load to heal. A short period of relative rest is fine, but prolonged offloading weakens the tendon further.
- Aggressive stretching: Stretching a painful tendon under compression can provoke symptoms, especially for insertional tendinopathies (where the tendon meets the bone).
- Repeatedly testing the tendon: Many patients check their symptoms throughout the day by bouncing on their heels or pressing the tendon. This sensitises the area and slows recovery.
- Ignoring the warning signs: A tendon that is repeatedly provoked without adequate recovery will progress along the pathology continuum. Address it early.
As someone who lives and breathes the gym myself, I know how important it is to have the right environment to train in — especially when you’re recovering from a tendon injury. That’s why I’m particularly proud of our fully equipped gym at our Esher and Southwark clinics.
How Long Will It Take?
Honestly? Tendons are slow to heal — and this is one of the hardest things to communicate to patients who are used to soft tissue injuries resolving in a few weeks.
A reactive tendinopathy caught early might resolve in 6–8 weeks with good management. A more established tendinopathy with significant dysrepair or degeneration may take 3–6 months of consistent, progressive rehabilitation.
The key is that progress doesn’t have to mean pain-free. We use simple monitoring tools — like the Visual Analogue Scale or the VISA questionnaire — to track your symptoms and guide progression. Some discomfort during rehab is expected and acceptable; sharp spikes in pain lasting beyond 24 hours after exercise are a signal to pull back.
A Final Word From Me

Tendinopathy is genuinely one of my favourite conditions to treat — partly because the science is fascinating, and partly because when patients commit to the process, the results can be remarkable. I’ve seen people go from barely being able to walk without heel pain to completing marathons. I’ve watched gym-goers with years of patellar tendon trouble get back to squatting heavy again.
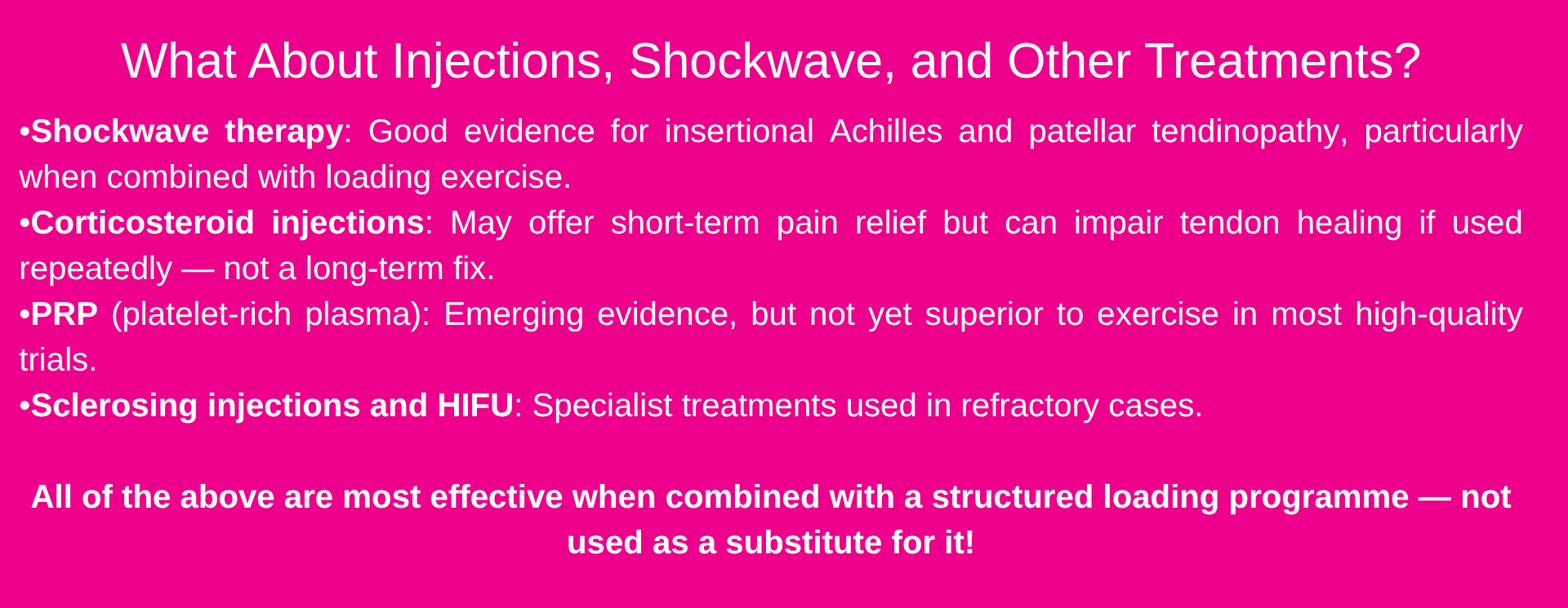
The secret is not a magic injection or a passive treatment. It’s smart, progressive loading — guided by someone who understands tendon biology. That’s what we do at Vitality.
If you’re dealing with a stubborn tendon that isn’t responding to what you’ve tried so far, come and see us. We’ll assess what’s going on, explain exactly what’s happening, and build you a programme that gets you back to doing what you love.
Book your tendinopathy assessment: vitality-physio.co.uk
Clinics in Southwark (SE1) and Esher (KT10)
This article is for educational purposes and does not constitute personalised medical advice. If you have symptoms, please consult a qualified physiotherapist or healthcare professional.







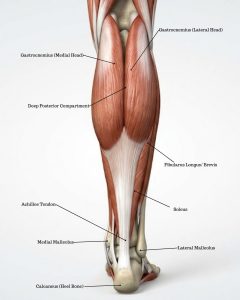 The Achilles tendon is the largest and strongest tendon in the body. It connects the calf muscle complex — the gastrocnemius (medial and lateral heads) and soleus — to the heel bone (calcaneus), forming a thick, powerful structure that stores and releases energy with every step. It is central to walking, running, jumping, and pushing off the foot.
The Achilles tendon is the largest and strongest tendon in the body. It connects the calf muscle complex — the gastrocnemius (medial and lateral heads) and soleus — to the heel bone (calcaneus), forming a thick, powerful structure that stores and releases energy with every step. It is central to walking, running, jumping, and pushing off the foot. Load management The first step is to reduce aggravating activities to a level the tendon can tolerate, while maintaining as much training as possible. Complete rest is rarely helpful and may slow recovery.
Load management The first step is to reduce aggravating activities to a level the tendon can tolerate, while maintaining as much training as possible. Complete rest is rarely helpful and may slow recovery.