Subacromial Impingement: Symptoms, Causes & Treatment
Subacromial impingement is one of the most common causes of shoulder pain, accounting for up to 65% of all shoulder complaints seen in clinical practice. If you’ve noticed pain when reaching overhead, lying on your shoulder at night, or performing a serve or golf swing, subacromial impingement could be the reason.
The good news is that the vast majority of people recover well with the right physiotherapy, without needing surgery. At Vitality Physiotherapy in Southwark, London SE1, we assess and treat subacromial impingement every week, helping active people get back to the sport and daily life they love.
What Is Subacromial Impingement?
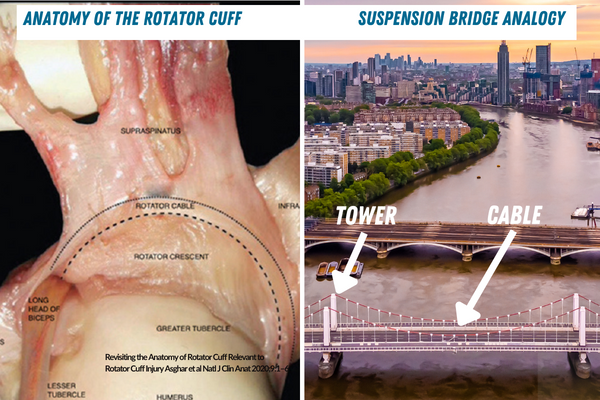
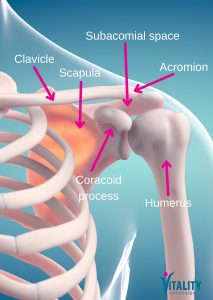 The shoulder is a remarkably mobile joint — but that mobility comes at a cost. A small space called the subacromial space runs between the top of the upper arm bone (humerus) and a bony arch formed by the shoulder blade (the acromion). Running through this space are the tendons of the rotator cuff and a small fluid-filled cushion called the subacromial bursa.
The shoulder is a remarkably mobile joint — but that mobility comes at a cost. A small space called the subacromial space runs between the top of the upper arm bone (humerus) and a bony arch formed by the shoulder blade (the acromion). Running through this space are the tendons of the rotator cuff and a small fluid-filled cushion called the subacromial bursa.
Subacromial impingement occurs when these soft tissue structures become compressed or irritated within this narrow space, typically during arm movements — especially lifting the arm to the side or overhead. Over time, repeated impingement can cause inflammation, pain, and in some cases, partial or full rotator cuff tears.
A note on terminology: You may come across clinicians and researchers who argue that “impingement” is an imprecise — or even misleading — label. Their point is a fair one: a degree of subacromial compression is a normal part of shoulder movement, and it is only when the structures within that space become pathological that pain arises. For this reason, terms such as subacromial pain syndrome or rotator cuff-related shoulder pain are increasingly preferred in clinical literature. We use the term “subacromial impingement” here because it remains the most widely recognised by patients, but the most important thing — whatever the label — is identifying and addressing what is actually driving your pain.
Symptoms of Subacromial Impingement
Symptoms vary between individuals, but the most common complaints include:
- Pain on the top and outer side of the shoulder, which may radiate down the upper arm
- A “painful arc” — pain that occurs when raising the arm between roughly 60° and 120° of elevation
- Night pain, particularly when lying on the affected shoulder
- Pain with overhead activities such as reaching to a shelf or dressing
- Reduced shoulder strength or difficulty sustaining overhead movements
- Pain during sport — for example, the forward swing when serving in tennis, or the backswing in golf
In some cases, you may also notice a catching or clicking sensation as the arm moves. If weakness is significant, or if pain came on after a fall or direct impact, a rotator cuff tear should be ruled out.
What Causes Subacromial Impingement?
Impingement can develop gradually through wear and overuse, or more suddenly following a change in training load or a specific injury. Common contributing factors include:
 Structural factors
Structural factors
 Structural factors
Structural factors- Bony spurs (osteophytes) on the underside of the acromion, which narrow the subacromial space
- An hooked or curved acromion shape (Type II or III), which is associated with higher impingement rates
- Calcific tendinitis — calcium deposits within the rotator cuff tendon
Functional and movement factors
- Rotator cuff weakness or muscle imbalance, particularly of the external rotators
- Poor scapular control — the shoulder blade fails to rotate or tilt correctly during arm elevation
- Postural habits that contribute to a rounded upper back and forward head position
- Sudden increases in training load, repetitive overhead activity, or technique errors in sport
It is worth noting that structural findings on imaging do not always correlate with pain. Many people have bony spurs or an hooked acromion and no symptoms at all, which is why treatment focuses on what’s driving your pain rather than what a scan shows
How Is Subacromial Impingement Diagnosed?
Diagnosis is primarily clinical, meaning a thorough physical assessment by a physiotherapist or clinician is the most important step. Your physiotherapist will carry out:
- A detailed history of your symptoms, activity levels, and aggravating factors
- Range of motion testing to identify painful arcs and movement restrictions
- Strength and rotator cuff testing to assess the integrity of the cuff muscles
- Specific orthopaedic tests, such as Hawkins-Kennedy and Neer’s tests, to reproduce impingement signs
- Scapular and postural assessment to identify contributing movement dysfunction
Imaging such as ultrasound or MRI may be requested if a rotator cuff tear is suspected, or if symptoms are not progressing as expected with treatment. X-ray can identify bony spurs or calcification but does not show soft tissue structures.
Treatment for Subacromial Impingement
Most specialist guidelines — including those from NICE and the British Elbow and Shoulder Society — recommend physiotherapy as the first-line treatment for subacromial impingement. Surgery is generally only considered if conservative management over three to six months has not produced sufficient improvement.
What physiotherapy involves
At Vitality Physiotherapy, we take a whole-body approach. We don’t just treat the painful shoulder in isolation — we assess the entire kinematic chain, including the thoracic spine, scapula, and hip and core stability, all of which can contribute to shoulder dysfunction.
Your treatment plan may include:
- A targeted rotator cuff strengthening programme, progressed according to your goals and tolerance
- Scapular stabilisation exercises to restore efficient shoulder blade movement
- Thoracic mobility work to improve upper back extension and rotation
- Manual therapy — joint mobilisation or soft tissue work — to reduce pain and improve movement
- Postural re-education and workstation or technique advice where relevant
- Kinesiology taping as an adjunct to support the shoulder and reduce pain during activity
- Sports-specific rehabilitation, working in collaboration with your coach or personal trainer where appropriate
How long does recovery take?
 Recovery time varies depending on the severity of the impingement and any underlying structural changes. Most people with subacromial impingement see significant improvement within 6–12 weeks of consistent physiotherapy. Those with a concurrent partial rotator cuff tear, significant structural changes, or a longer history of symptoms may take longer.
Recovery time varies depending on the severity of the impingement and any underlying structural changes. Most people with subacromial impingement see significant improvement within 6–12 weeks of consistent physiotherapy. Those with a concurrent partial rotator cuff tear, significant structural changes, or a longer history of symptoms may take longer.
The key to a good outcome is early assessment, a well-structured rehabilitation programme, and addressing the root cause — not just the pain.
Will I need surgery?
The majority of people do not need surgery. A large body of evidence, including the influential CSAW trial, has shown that for most patients, subacromial decompression surgery provides no significant advantage over a well-delivered physiotherapy programme. This reinforces why early, expert physiotherapy is so important.
If surgery is recommended by your consultant after conservative treatment, your physiotherapist will work closely with your surgeon to optimise your pre-operative strength and your post-operative rehabilitation.
Struggling with shoulder pain? Book an appointment at our Southwark (SE1) clinic and get a thorough assessment today.
What Can You Do in the Meantime?
While you are awaiting assessment or in the early stages of treatment, the following can help manage symptoms:
- Modify — don’t stop — activity. Avoid positions that reproduce sharp pain, but keep moving within a comfortable range.
- Sleep position: try sleeping on your unaffected side with a pillow supporting the painful arm in front of you.
- Ice or heat: short-term use of ice packs (10–15 minutes) can help in acute flare-ups; some people prefer warmth for ongoing stiffness.
- Anti-inflammatory medication: over-the-counter NSAIDs such as ibuprofen can provide short-term pain relief if appropriate for you — always check with your pharmacist or GP.
Please avoid self-diagnosing and attempting to self-treat without professional guidance. Many shoulder conditions share similar symptoms, and an accurate diagnosis will ensure you follow the right programme for your specific presentation.
Frequently Asked Questions
Is subacromial impingement the same as a rotator cuff tear?
Not exactly. Subacromial impingement refers to compression of the rotator cuff tendons (and bursa) within the subacromial space. A rotator cuff tear is a structural injury to the tendon fibres themselves, which can occur as a result of prolonged impingement or from a sudden traumatic event. The two conditions can co-exist, which is why a thorough assessment is important.
Can I still exercise with subacromial impingement?
Yes — in most cases, staying active is beneficial. The key is modifying your exercise to avoid pain-provocative movements while you work on the underlying cause. Your physiotherapist will guide you through what is safe to continue and what to temporarily adjust.
Do I need a GP referral to see a physiotherapist?
No. In the UK you can self-refer directly to a physiotherapist. At Vitality Physiotherapy in London SE1, you can book an initial assessment online without a GP referral. If imaging or onward referral is needed, we will advise you accordingly.
Ready to get your shoulder assessed?
Our experienced physiotherapists at Vitality Physiotherapy, Southwark SE1 are specialists in sports and musculoskeletal physiotherapy. We offer same-week appointments and a thorough, personalised assessment to get you on the right path.
→ Book your appointment online | Call us: 0207 193 9928
Last reviewed: February 2026 | Vitality Physiotherapy Ltd