ACL injuries

We've all come across a friend or famous athlete who has had their season cut short through an ill-timed knee twist and alongside the dreaded "popping" sound. When this happens, it can be daunting.
Understanding ACL injury and knowing what steps to take to recover will help you get back to the sport you love sooner. As mentioned in our ACL tear article, the ACL is one of the main ligaments controlling the stability of your knee, and injuries to the ACL occur more frequently in sports involving landing and pivoting actions like football, netball, or skiing.
Diagnosis of ACL Injuries
The Lachman Test
John Lachman (1919-2007) was an orthopaedic surgeon at Temple University in Philadelphia who invented the technique. It's considered the most reliable way to diagnose an ACL injury. It is used by Physios and Surgeons the world over.
How is the Lachman test performed?
The Lachman test is performed like this:
- Lie flat on your back. Relaxed, with legs straight.
- Your Physio places your knee in a slightly bent (and sometimes rotated) position.
- One hand is on the back of your lower leg (just under your knee joint), and the other is on the front of your thigh.
- They then pull your shin forwards firmly while stabilising your thigh.
Why do we do the Lachman test?
To measure the endpoint and joint laxity.
The endpoint is where the end of the joint movement is felt as the shin is pulled forward. If this endpoint feels further away than what's expected, then this may indicate an injured ACL.
Joint laxity is the general feel of your joint movement and the sense of how lax (or loose) your ACL feels compared to your other knee.
Grading ACL tears with the Lachman test:
- Normal. There's no difference in movement or laxity between your left and right knees.
- Mild (grade 1). There's slightly more (about 2-5mm) movement than in your other knee.
- Moderate (grade 2). There's moderately more (about 5 to 10 mm) movement than in your other knee.
- Severe (grade 3). There's much more (10 to 15 mm) movement than in your other knee.
Because we're all different and have varying baselines of "stiffness", the test should be done on your other leg too. This will give the Physio an accurate idea of what's typical for your joint.
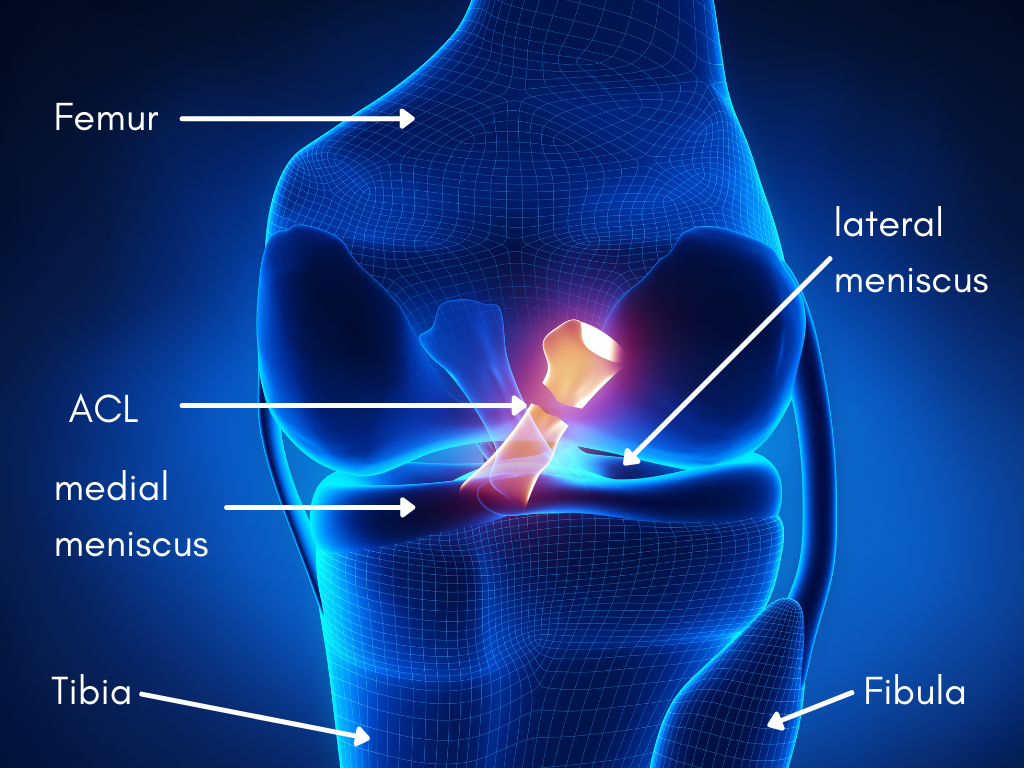
Anatomy of the L knee showing a ruptured ACL
The Pivot Shift test
How is the pivot shift test performed?
1. Lie flat on your back. Relaxed, with legs straight.
2. The Physio places one hand on your heel and the other just below the outer side of your knee.
3. They apply pressure to the outside of your knee while internally rotating your lower leg and bending and straightening your knee.
The test is positive if your lower leg sinks backward when the knee is bent at 30-40 degrees. Sometimes a 'clunk' can be heard when this happens.
Treatment options for ACL tears
There are two treatment options for an ACL injury: Conservative or surgical management.
Your age, previous injury, and fitness and rehab goals should be considered when deciding the best route to follow.
Conservative management
Conservative or non-surgical management involves a period of Physiotherapy treatment to restore your knee function to pre-injury level.
Surgical management
Having ACL surgery usually requires a minimum of 9 months of rehab tailored towards getting you back into your sport. This may sound like a long time, but returning to sport too early can have negative implications. Mainly increasing your risk of re-injury.
ACL Surgery
What surgery is there for ACL tears, and what you can expect?
The most common type of ACL surgery is a reconstruction of a new tendon called a graft. This is typically a minimally invasive procedure done via keyhole surgery using an arthroscope (a small camera through which your surgeon passes tiny surgical instruments). First, the damaged ACL is removed, and then the graft is attached in its place. There are different types of grafts. They include:
- Autografts - Formed from tissues taken from another part of your body (like tendon tissue strands from your hamstring or patella tendon)
- Allograft - Formed from tissues taken from another person's body
- Synthetic - Formed from an artificial source or donor.
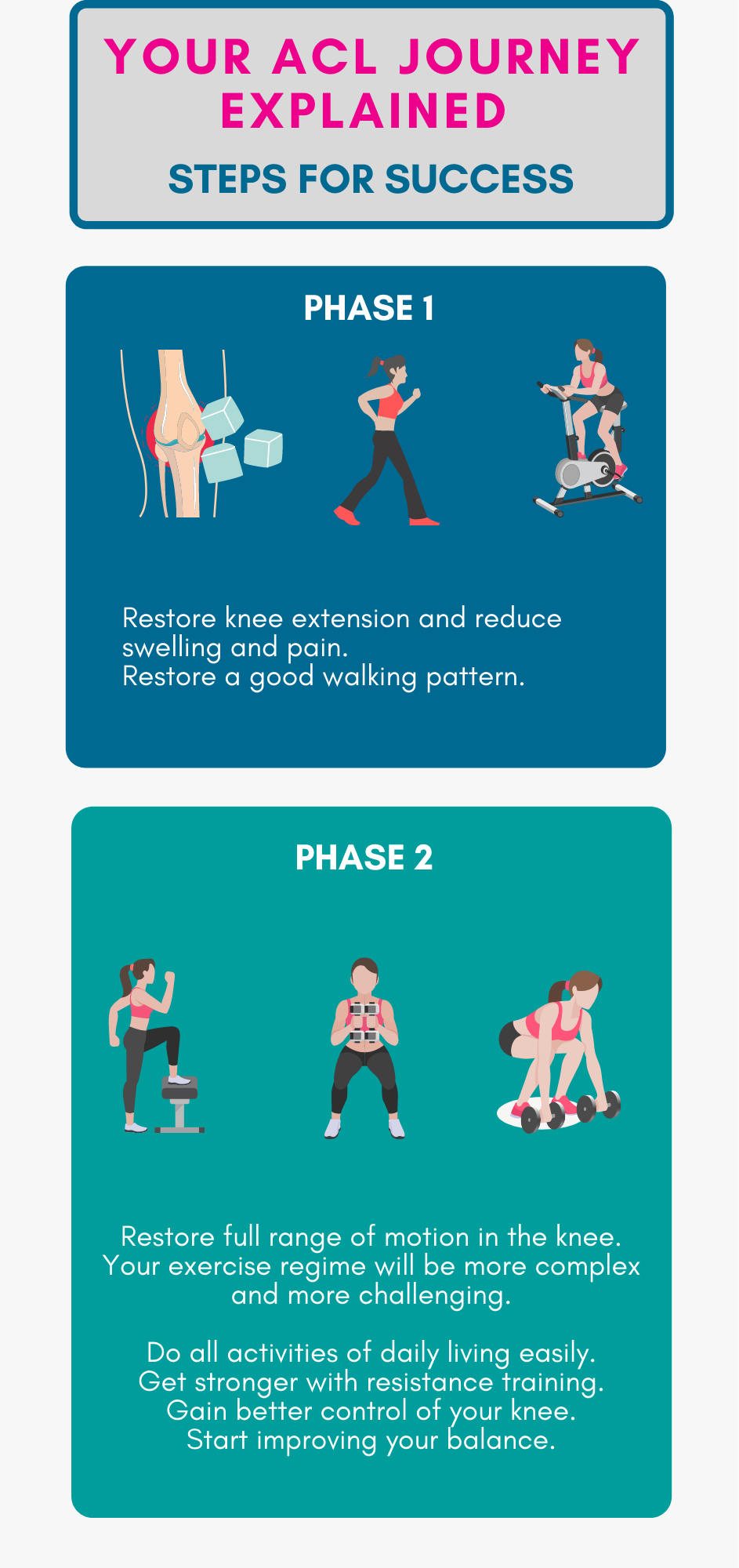
Rehab is paramount to your ACL recovery (with or without surgery) . Without rehab, ACL surgery is meaningless. All the top knee surgeons agree. Your ACL rehab determines the success of your recovery. We recommend an evidence-based programme that's divided into four progressive phases. In our experience, this process takes 9 to 18 months to complete.