Everything you need to know about recovering well after having a baby – backed by clinical evidence, written in plain English.
Having a baby is one of the most significant physical events a woman’s body will ever go through. Yet postnatal recovery is often under-discussed, under-resourced, and misunderstood. This guide answers the questions we hear most often in clinic — honestly, practically, and with your long-term health in mind.
Written by Tamara Figaji, Associate Women’s Health Sports Physiotherapist at Vitality Physiotherapy.
 Q1 When should I start pelvic floor exercises after birth?
Q1 When should I start pelvic floor exercises after birth?
This is one of the most common questions we’re asked — and the short answer is: sooner than most people think.
The first 24 hours
Provided you feel comfortable and there are no complications, gentle pelvic floor contractions can begin within the first day after birth — whether you’ve had a vaginal delivery or a caesarean section. In the early days, these aren’t about ‘getting your pelvic floor back’; they’re about encouraging circulation, reducing swelling, and beginning the healing process.
Even if you can’t feel much at first — especially after a difficult delivery or if you’ve had stitches — that’s normal. The nerve supply to the pelvic floor can be temporarily affected by birth, so reduced sensation doesn’t mean nothing is happening.
The first 6 weeks
During this period, focus on low-intensity exercises. These include:
- Slow, held contractions: gently lift and squeeze, hold for up to 10 seconds, then fully release
- Quick contractions: short squeeze and releases to activate fast-twitch muscle fibres
- Deep breathing with diaphragmatic engagement: your pelvic floor and diaphragm work together
Equally important is the release. Many women are so focused on ‘tightening up’ that they forget the pelvic floor must also fully relax. A pelvic floor that cannot let go is just as problematic as one that is weak.
| ⚠️ Important: Not all pelvic floor problems mean weakness Some women experience pelvic floor tension or overactivity after birth, where muscles are tight and unable to relax. Doing more squeezing exercises in this case can make symptoms worse. If you’re experiencing pain, pressure, difficulty with bowel movements, or pain during sex, please seek assessment before continuing with generic pelvic floor programmes. |
When to progress
From 6–12 weeks, as your body heals and you receive clearance at your postnatal check, you can begin building intensity and duration. This is also the time to start thinking about returning to more demanding activity — we’ll cover running specifically in Q5.
| ✅ Clinical recommendation Every woman who has given birth — regardless of delivery type, age, or symptom status — would benefit from a pelvic floor assessment with a specialist physiotherapist at or after 6-8 weeks postnatal. This is standard practice in France and many other countries, and something we advocate strongly for in the UK. |
Q2 What is a Mummy MOT?
The term ‘Mummy MOT’ has become widely used, but it’s worth understanding exactly what it involves — and why it’s so valuable.
What it is
A Mummy MOT is a specialist postnatal assessment carried out by a trained women’s health physiotherapist, typically from around 6-8 weeks after birth, ideally after GP postnatal check. It’s a thorough, evidence-based review of your postnatal recovery that covers:
- Pelvic floor muscle function — strength, coordination, relaxation and endurance
- Abdominal muscle assessment — including checking for diastasis recti (tummy gap)
- Posture, breathing and movement patterns
- Scar tissue assessment (perineal or caesarean)
- Return-to-activity guidance based on your individual findings
Why it matters
The standard NHS 6- 8week postnatal check is carried out by a GP, and while valuable, it typically does not include a pelvic floor examination or musculoskeletal assessment. For many women, this means problems go undetected — sometimes for years.
Research suggests that up to 1 in 3 women experience pelvic floor dysfunction after childbirth, including urinary leakage, pelvic organ prolapse, or pain. The majority never seek help, often because they believe these symptoms are ‘normal’ or ‘just part of having a baby.’
They are common — but they are not inevitable, and they are treatable.
| 💬 A note from Tamara In clinic, I see many women who have been silently managing symptoms for months or years before coming to see us. A Mummy MOT gives us the full picture of how your body is recovering — and means we can create a personalised plan to get you back to doing everything you love, safely and confidently. |
When to book
We recommend booking your Mummy MOT from 6 – 8 weeks postnatal for vaginal deliveries, or from 8–10 weeks following a caesarean section, or after your GP postnatal check for both. However, assessments can be carried out at any point after this time — it is never too late to be assessed, even years after giving birth.
| What’s included | What you’ll receive |
| 60-minute one-to-one assessment | Personalised exercise programme |
| Pelvic floor internal examination (with consent) | Scar management advice if applicable |
| Diastasis recti check | Graded return-to-activity plan |
| Full movement & posture review | Referral or onward support if needed |
Q3 Why do I still look pregnant months after giving birth?
This is something many women worry about and feel embarrassed to ask. The good news is that there are clear physiological explanations — and in most cases, effective things you can do about it.
Your uterus needs time to involute
Immediately after birth, your uterus begins the process of involution — shrinking back towards its pre-pregnancy size. This takes approximately 6 weeks. During this period, a rounded lower abdomen is entirely normal and expected.
Abdominal muscles have been stretched
During pregnancy, the rectus abdominis muscles (your ‘six-pack’ muscles) are stretched apart to accommodate your growing baby. The connective tissue between them — the linea alba — widens in all pregnancies to some degree. This is called diastasis recti, which we cover in detail in Q4.
A persistent domed or coned appearance to the abdomen, particularly when sitting up or under exertion, is often a sign of diastasis recti that needs attention.
Skin and fascia laxity
The skin and deeper fascial layers of the abdomen have been under sustained stretch for nine months. Skin has limited elasticity after this level of sustained stretch, particularly with larger babies, multiple pregnancies, or when significant weight change has occurred. Some degree of laxity may remain permanently — and this is a completely normal part of having carried a baby.
Posture and muscle inhibition
Postnatal posture changes — often exacerbated by feeding positions, carrying, and sleep deprivation — can make the abdomen appear more prominent. When deep core muscles such as the transversus abdominis are not functioning optimally, the abdominal wall may have a more lax appearance.
Fluid retention
Some women retain fluid for several weeks postnatally, which can contribute to a swollen or puffy appearance across the abdomen and lower body. Staying well hydrated, moving gently, and elevating the legs when resting can help.
| When to seek advice If you are experiencing a persistent domed or asymmetric appearance to your abdomen, particularly when you cough, sneeze, or sit up, or if your abdomen feels weak or unsupported when you move, please book a postnatal physiotherapy assessment. These presentations can be assessed and treated effectively with the right guidance. |
Q4 How do I close a tummy gap (diastasis recti)?
Diastasis recti — the separation of the rectus abdominis muscles — is one of the most searched postnatal topics, and also one of the most misunderstood. Here’s what you actually need to know.
First: what it is and isn’t
Diastasis recti is a widening of the inter-recti distance (IRD) — the space between the two columns of abdominal muscle. A small degree of separation is normal in all pregnancies. Clinically, we tend to consider a distance of 2cm or more, combined with impaired function of the connective tissue (poor tension and depth), as requiring intervention.
Crucially: the goal is not always to ‘close the gap.’ A narrow gap with poor tissue tension and function is more problematic than a slightly wider gap with good tension and load transfer. What matters most is how well the abdominal wall functions as a unit.
What makes it worse
Certain activities can place excessive load on the linea alba and impede recovery. In the early postnatal period, avoid:
- Traditional sit-ups, crunches, or double-leg raises
- Heavy lifting without breath and bracing technique
- High-impact exercise before adequate healing
- Planks and push-ups if you notice coning or doming of the midline
This doesn’t mean these exercises are permanently off-limits — it means timing and progression matter.
What helps
Recovery from diastasis recti is graduated and individual. A well-structured programme typically includes:
- Breathing and deep core activation: learning to engage the transversus abdominis and coordinate breath with movement is the foundation of diastasis rehabilitation
- Progressive loading: gradually reintroducing load through the core as tissue tension and function improve
- Postural optimisation: addressing compensatory patterns that increase intra-abdominal pressure
- Functional movement retraining: returning to everyday tasks — lifting, carrying, getting up from the floor — with optimal mechanics
Realistic expectations
With appropriate intervention, most women see significant functional improvement and reduction in gap width. However, some degree of laxity may remain — and this is not a failure. Many women with a measurable IRD have no functional symptoms whatsoever.
If you’ve been told you have diastasis recti, or if you notice the classic signs — coning at the midline, lower back pain, pelvic instability, or difficulty generating core tension — a specialist physiotherapy assessment will give you a clear, personalised plan.
| 📋 What to expect at a diastasis assessment At Vitality Physiotherapy, we assess inter-recti distance, tissue quality (tension and depth), load transfer and abdominal function through movement. From this, we create a structured rehabilitation programme that progresses at the right pace for your body and your goals — whether that’s returning to yoga, lifting your toddler, or running a 10K. |
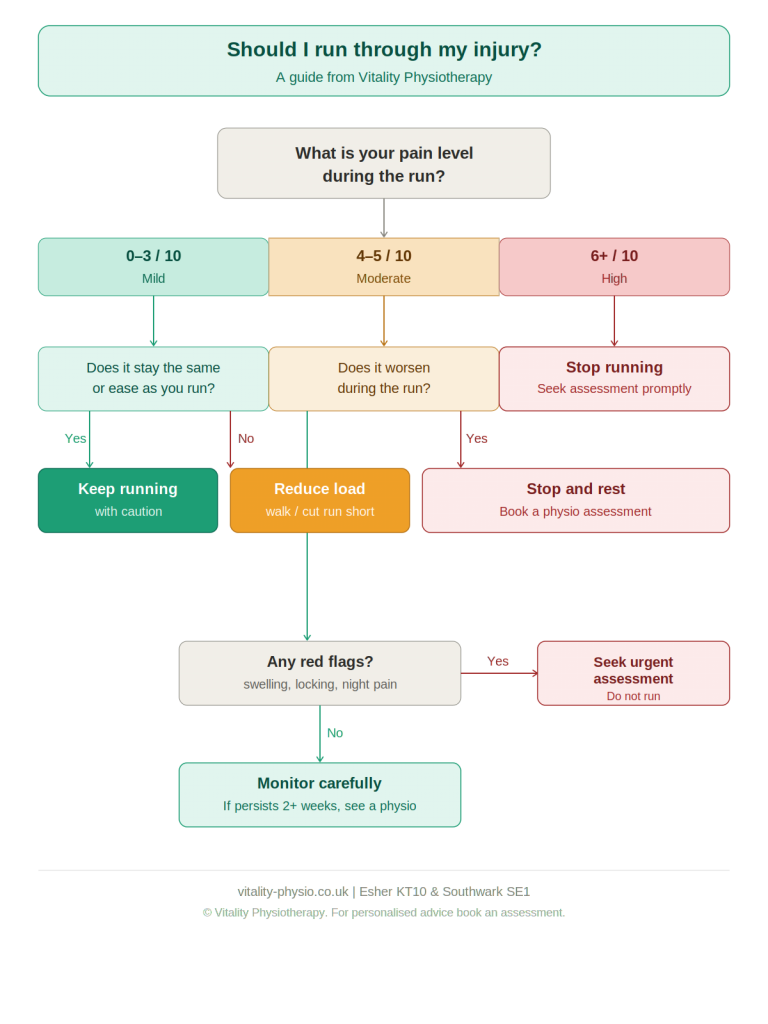
Q5 Is it safe to run after having a baby?
Running is one of the most popular forms of exercise women want to return to after having a baby. And the answer to whether it’s safe is: yes — but with the right preparation, at the right time.
Why the timing matters
Running is a high-impact activity. Every stride loads the pelvic floor with forces of 1.5–2.5 times your body weight. This is a significant demand to place on tissues that are still recovering from pregnancy and birth.
The landmark guidelines published by specialist physiotherapists Groom, Donnelly and Brockwell — widely adopted in clinical practice — recommend that women wait until at least 12 weeks postnatal before returning to running, and that this return is graduated and symptom-guided.
Signs that you may not be ready
Before returning to running, you should be free of the following symptoms during everyday activity:
- Urinary leakage (stress incontinence)
- Pelvic heaviness, pressure, or bulging
- Pelvic girdle or lower back pain
- Abdominal coning or doming
- Difficulty with single-leg activities such as stairs or walking
If any of these are present, these are signals to address the underlying issue before introducing running loads.
The readiness tests
Before beginning a return-to-run programme, you should comfortably be able to:
- Walk briskly for 30 minutes without symptoms
- Single-leg balance for 10 seconds each side
- 20 single-leg calf raises without discomfort
- 10 single-leg bridges on each side
- 20 forward bounds (low-impact hopping), symptom-free
Building back up
A graduated return-to-run programme — similar in structure to Couch to 5K — is the safest approach. Alternate running and walking, begin on softer surfaces, and pay close attention to any symptoms during or after sessions.
| Week | Session structure | Symptom check |
| 1 | 1 min run / 2 min walk × 8 | Leakage, heaviness, pain? |
| 2 | 2 min run / 2 min walk × 6 | Any new symptoms? |
| 3 | 3 min run / 1 min walk × 6 | Confidence improving? |
| 4 | 5 min run / 1 min walk × 5 | Continuous running felt ok? |
| 5–6 | 10 min run / 1 min walk × 3 | Assess for full return |
If symptoms occur during or within 24 hours of a run, step back one week in the programme and reassess. Persistent symptoms should prompt a physiotherapy review before continuing.
| 🏃 Running with a pelvic floor that’s ready At Vitality Physiotherapy, we offer specialist return-to-running assessments that combine pelvic floor evaluation with a movement and gait screen. This gives you a clear picture of your readiness, a tailored programme, and the confidence to run without worrying about your symptoms. Whether you’re aiming for your first 5K or returning to half-marathon training, we can help you get there safely. |
| Ready to start your recovery properly? Clinics in London (SE1) and Surrey (KT10 Esher) Book a Mummy MOT or postnatal physiotherapy assessment vitality-physio.co.uk |
About the author
Tamara Figaji is an Associate Women’s Health Sports Physiotherapist at Vitality Physiotherapy, specialising in postnatal recovery, pelvic floor rehabilitation, and return-to-sport. She works with women at both the London (SE1) and Surrey (KT10 Esher) clinics.
The information in this article is for educational purposes and does not constitute individual medical advice. If you are experiencing symptoms or have concerns about your postnatal recovery, please book an assessment with a

 Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.
Here is the part that gets overlooked in most conversations about back pain: capacity is trainable. When load is introduced progressively, tissues respond. Muscles strengthen. Bones become denser. Tendons grow more robust. Discs adapt. The body is not a static, fragile structure — it is a dynamic, responsive system.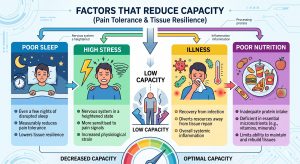 The factors that reduce capacity include:
The factors that reduce capacity include:

 Q1 When should I start pelvic floor exercises after birth?
Q1 When should I start pelvic floor exercises after birth? The term ‘Mummy MOT’ has become widely used, but it’s worth understanding exactly what it involves — and why it’s so valuable.
The term ‘Mummy MOT’ has become widely used, but it’s worth understanding exactly what it involves — and why it’s so valuable. Q4 How do I close a tummy gap (diastasis recti)?
Q4 How do I close a tummy gap (diastasis recti)? Q5 Is it safe to run after having a baby?
Q5 Is it safe to run after having a baby?



 Una instantánea de la carrera mundial de vacunas dirigidas contra el SARS-CoV-2 y la pandemia COVID-19. Parte delantera. Pharmacol. 11:937.Funk CD, Laferrière C and Ardakani A (2020) A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic. Front. Pharmacol. 11:937.https://doi.org/10.3389/fphar.2020.00937, CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=99473789")